


My latest response to
. If you missed the previous correspondence please see this page.Dear Clare,
Thank you for your last response.
I set out to gain a better understanding of your views on what happened in late 2019 and early 2020, especially with regard to your belief that SARS-CoV-2 is a virus and is manmade.
After reading your replies - and now having read your book in full - I have a better grasp on your perspective, which (as you’re aware) is very different from mine. An article you and I have each cited is emblematic: You cited “The Unacceptable Risks of a Man-Made Pandemic” (Klotz & Sylvester, 2012) for its estimate of a laboratory leak affecting 5-15% of people; I footnoted the article as a clear example of a ‘pandemic ghost story.’
Interviews, articles, and tweets show that you and I experienced the first six months of 2020 very differently, had different concerns, and reacted differently to abrogations of fundamental liberties. Time machines and body-switching are impossible, so - like I said of my father’s 9/11 - on that front there can only ever be empathy and (someday, hopefully) a shared perspective on what the evils were and how they can be exposed and prevented from happening again.
We agree officials lied about dangers of a new disease and about the safety and efficacy of the COVID shot. I see the entire escapade as staged and fraudulent; whereas you regard elements of the official story and its never-ending series of surface-level “costume changes” as truthful. For example, I don’t consider hubristic, grandiose ideas in grant proposals as evidence of anything being achieved or realized. Research dollars were being spent on scouring bat caves without any evidence whatsoever of transmission from bats to humans (or bats to humans via intermediary host). A well-funded fool’s errand is still a fool’s errand.
Some of the points I would make in response to your view on viruses and SARS-CoV-2 are in an article I wrote last week which features excerpts from correspondence with an academic virologist. I hope you’ll read and consider what both he and I have said. His assumption and yours is that viruses “enter” the body “from the outside” versus being something that is produced “from within.”
It took me longer than it’s taken some, but I now highly doubt viruses are what we have been led to believe or that (what you termed) “the virus model” and “conventional model of virus attack” are correct. I concur with distinctions the legally-minded Katherine Watt and Jonathan Engler have made, appreciate Stefan Lanka’s orientation (as articulated here), and lean toward the things classified as viruses being an endogenous phenomenon and SARS-CoV-2 a computer-facilitated constructed entity.1
As stated here, while I don’t consider “There are no viruses!” a rhetorically-superior or necessarily more persuasive technique in the effort to undermine the WHO et al’s COVID Era claims, the “No Virus” view raises scientifically and medically important questions that are clearly being avoided by those who hold and continue to advocate a “Last Pandemic/Next Pandemic” view like this one.
If viruses are “a thing,” I see no reason to believe scientists can create or adulterate a viable version with the functions proposed, irrespective of “gain”. You disagreed with this view, whereas I agreed (here and here), so we are at an impasse. I commend to you the numbered summary points in this essay.
Ben Marten raised and addressed the question of whether viral genomics are evidence of spread. You’ve said he made some valid points, without specifying which ones. I have no expertise in genomics but, as a result of the COVID event, hold the enterprise in low regard insofar as bettering the health and welfare of humankind.2
You’ve pointed to the UK REACT-2 antibody study as evidence that a novel coronavirus causative of a unique disease began making the rounds in late 2019/early 2020. We reviewed the study, identified numerous flaws, and reject that assertion. Other points I would make about the utility of serology testing for pinpointing the “arrival” and trajectory of SARS-CoV-2 are here and here.
Regarding your proposed mechanism of rapid “spread” across the world, many things you characterize as “observations” are not observations scientifically-speaking because they are not directly observed by the senses but inferred from the results of imprecise, unreliable, and possibly invalid methods that are subject to over-/mis-/mal-interpretation.
Being able to approximate or achieve “something” in a lab or under controlled or simulated conditions does not necessarily mean a real-world process or mechanism is being demonstrated. I’m again with Sunetra Gupta on this when she said, “I don't think you can make something in the lab that's going to be able to compete successfully with what's out in the world.” You seem to accept this with respect to doing things with cells in a lab but not when it comes to ‘spread.’
The studies reporting virus detection far from humans are intriguing, and the measurement approaches beyond my expertise to evaluate, but they raise more questions about what viruses are, exactly. Also, is there a reason we don’t see comparable studies of the air “on the ground” in London or Chicago?
You believe
aerosol transmission occurs when people exhale virus-containing particles into the air, where they can remain for 'very long periods of time.' 'Spread' is extremely fast, and the viruses and its variants 'traverse the world' independently of air travel. Most transmission occurs at night—when people are typically indoors or asleep. Dosage of virus in the air will also rise and fall with a wave.
Is the idea that viruses are in air in my neighborhood - and more so at night? Can we sample the air and find SARS-CoV-2? People tend to be indoors more at night, but is there evidence that more ‘viral’ transmission occurs at night?
The only way I can see ‘viruses’ traversing the world in the manner and with the speed you’ve suggested is via some kind of coordinated ‘chemtrails’ effort, which I would characterize as dispersal, versus viruses ‘behaving’ in a certain way.3 With ‘Dosage of virus in the air will also rise and fall with a wave,’ it sounds like you’re saying viral concentrations in the air are governed by intrinsic, seasonal wave dynamics. Are there studies which support this idea?
Speedy global detection of new variants and “crazy numbers” being sequenced is, at most, evidence of the potential presence of something - not evidence of “spread”. It’s very possible that the appearance of different variants was aided and abetted by changes to the “tests” themselves or other undisclosed factors.
Spread isn’t difficult to simulate via testing, and the “sudden appearance” of a virus cannot be divorced from the deployment of testing. This “magic trick” occurred with H1N1. It’s clear from U.S. data (below) that the positive tests for sequenced specimens influenza virus strains were winding down, concurrent with the advent of spring, when people tend to go to the hospital less, and then end of the active surveillance seasons.
Source: Setting the Stage for the Flu’s Disappearing Act (Hockett, 1 July 2023)
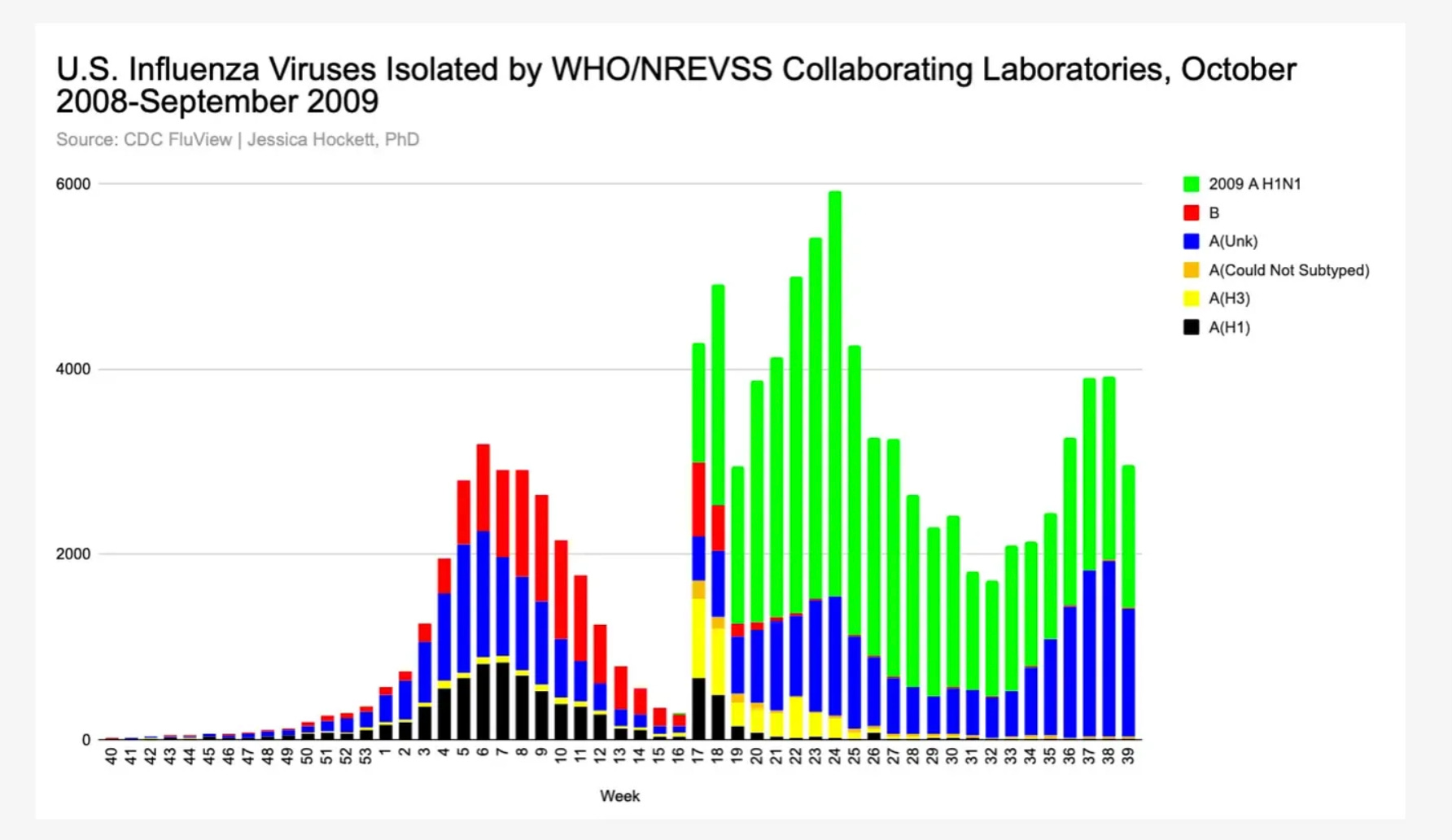
Then, the WHO et al sounded an alarm (without cause), people in and coming to the hospital were tested, and we see “the new thing” come online, as well as positives for the “old things” being resurrected from their “dormancy”. The “waves” we see in ILI visits and testing should not be interpreted as a function of viral behavior per se but of human behavior and decision-making and (on the part of some) intent to deceive. Non-viral stimuli triggered a change in people’s perception and, with the use of ‘novel’ tests, cast the specter of sudden spread of a freshly-emerged pathogen.
It’s the same thing with SARS-CoV-2. The virus *appeared* with testing. At most, something already there was identified, given a name, and a “test” (procedure) developed for finding “it”.4 The difference between H1N1 and SARS-CoV-2 is the latter relied on “damaged ships” in healthcare settings to trigger the appearance of a bomb-like pathogen.
In that vein, you’ve said three things I want to address head-on:
“The primary driver of spread [of SARS-CoV-2] is aerosol transmission because spread was too rapid, continued throughout lockdown reaching remote places and was unhindered by masking.”
The reason spread looks so rapid, far-reaching, and unstoppable is due to the sudden use of non-specific tests.
“The hospitalised population had peak infections at exactly the same time as the infections peaked in the community. If person to person spread was the cause of the peak then we would expect the hospital peak to occur after admissions from the community - that never happened.”
This is due to all of the testing that was taking place inside and outside of hospitals/care settings at very high rates, including repeat testing on the same patient/person.
“The peaks happen at predictable times of year. A wave of susceptiblity passing through the population makes sense of this but susceptibility to what? Virus in the air is still part of the equation.”
A “wave of susceptibility” is a wave of testing that reflects weather-related factors for hospitalization and deployment of various kinds of shots.
I urge you to read this study closely, including all supplemental materials, footnotes, and media. (It’s the one I highlighted in this presentation in May 2023, which I think you attended.)
A number of your propositions about SARS-CoV-2 are rooted in unproven cause/effect assumptions about influenza illness and the things called influenza viruses. For example, you said, “spikes of illness are caused by the same genetic variant” when no such relationship has ever been demonstrated. My read of Hope-Simpson is different from yours; I recommend John Dee’s series.
I realize spring is not out of season for flu in the UK (the same is true for most states here), but it’s still off-peak and the time when fewer people are tested for flu. I’m a bit confused as to what you’re saying regarding “a big difference in infection mortality rates” and I don’t see how you explain the gap between (for example) Berlin’s and London’s all-cause death curves. England bad, Germany good?
You said you think, even after eliminating deaths from other causes, “there was a virus which was causing more harm than an average seasonal respiratory virus” (i.e., it was adding risk of severe illness and death to some groups of people) but can’t explain why the virus wasn’t showing up in any data of any kind - including in places “hit hardest” like Bergamo and New York City - until an emergency was announced and mass testing deployed.
You mentioned knowing people who were “sicker with this than with normal seasonal respiratory viruses.” I’m guessing you are referring to periods after spring 2020. If you knew fellow citizens who became sick "with unusual respiratory illness during the “first wave” you’re the exception among Londoners I’ve spoken to, including a restaurant server.
At that time, we were living in Cook County (Chicago) - which reported a high number of deaths and “COVID” deaths. We didn’t personally know anyone who suddenly became sick with flu-like illness.
I’m sure you agree that, in any given year, some people will become “the sickest they’ve ever been”. Nocebo effect and psychogenic illness can’t be dismissed, nor can the compounding effects of societal upheaval, closures, anxiety, shots, etc. Personal experience isn’t evidentiary of novelty to humankind. The assumption that each “wave” of illness as asserted by positive tests and anecdotal reports of illness was driven by a single novel pathogen makes no sense and, even if it did, is impossible to disentangle. As Denis Rancourt explained very well, respiratory epidemics can (and do) occur without viral transmission.
While I understand the difficulty of estimating the excess deaths you believe would’ve occurred in spring 2020, because you’re not saying SARS-CoV-2 displaced deaths which would have occurred via influenza or other respiratory agents, the argument has to be stronger and must attempt to account for differences between specific locations.
Regarding the data in this surveillance report you referenced, I suggest requesting all raw underlying data for all graphs and seeing what you see. There is less support for your assertions than you think. Positive flu tests disappeared due to human interference - not visual interference or NPIs. I refer you to sections 24.5 and 24.6 in Norman Fenton and Martin Neil’s Fighting Goliath (alternatively, these articles) and my March 2023 thread. People control tests, testing, and the guidance around the use/misuse of those tests/that testing.
As to the advent of a new “disease,” we see no evidence of novelty, uniqueness, or SARS-CoV-2 being the singular causative agent of any symptoms or conditions.5 I’ve interviewed many doctors and nurses - including one of the more prolific. Not one has said they saw anything usual or resistant to typical treatment prior to testing and associated protocols being launched in their facilities. This presents a serious challenge to your view that, had nothing been done (e.g., no ‘detection of a new thing’, no ‘coordinated response’), a spike in all cause mortality would've been observed in some places.
You offered this blog post by Malcolm Kendrick as an example of a “frontline critically thinking GP describing his observations before anyone told him what to think.” Dr. Kendrick is listed as a member of an organization you co-lead, which biases your perspective. I note the date of his post (22 March 2025) falls between my 2 March 2025 reply to you and your 26 March 2025 response citing it.
Please refer to comments in this thread for my view on his reported experience. Nothing he says refutes my assertion that patterns in clinical observation did not precede doctors being told to associate a test result with certain things, and respond to those things with a given (democidal) protocol. Having analyzed the themes in what numerous medical voices elevated during the first 6-8 weeks of ‘the emergency’ were claiming, I can place Dr. Kendrick’s commentary - now and then - in the same bucket as those who seem to be following a kind of script of the ilk we would expect in a ‘wartime’ situation.
Thank you for clarifying that you think “the virus spread” began in Wuhan in autumn 2019 and proffering conditions. You said, “All that is required is for someone to be infected. From there, exponential replication of virus being breathed into night air is all that’s needed for spread. That does not preclude a deliberate release.”
Do you find it curious that this ‘exponential spread’ did not result in more Americans at the World Military Games being sickened? (Or is the explanation only some were susceptible?) The virus traversed the world in a matter of days, per your hypothesis, but waited until authorities gave it permission to do any damage - and even then only did so in certain places, with no plausible explanation for bizarre differences in timing and magnitude?
The most troubling implication of what you’re advancing is the idea that scientists are capable of creating a ‘virus’ that mimics what viruses (whatever those are) purportedly do. How does this not empower the pandemic/bioterrorism preparedness industry? Is the idea for me to tell my daughter, “Yes, viruses are everything we’ve been told they are and scientists created one that does what other viruses do, and ‘looked nasty on paper,’ but as long as we don’t ‘lockdown’ and create or mandate bad shots, we have nothing to fear”?
I find that incredibly misguided and entirely unsupported by any scientific or medical evidence.
More positively, you’ve said,
“No matter how bad something looks on paper, it is only as bad as it is in the real world.”
I agree and submit that efforts to uncover the truth should first and foremost consider what actually happened in the real world, versus on a screen.
Thank you again for helping me understand your views. Please forgive any typos or critical points I neglected to address. I’m happy to amend this digital letter as needed.
Regards,
Jessica Hockett
Clare did not acknowledge receipt of this letter and did not reply to an email requesting that she do so.
Added 20 August 2025, for reference.

Substack user Homer the Menace framed the big picture well in this comment. I trust you are familiar with the arguments and writings of many others in the "No Virus” corner of the arena, including but not limited to Mike Yeadon, Tom Cowan, Sam & Mark Bailey, Jaime Andrews, et al.
I am especially concerned by the integration of genomics with bad theology (here, for example) and suspect scientists have constructed a Tower of Babel.
Chemtrails are “not my rabbit hole,” as the saying goes, and my mention should not be construed as support or validation of hypotheses involving that ‘technique.’
A deeply flawed test, as you and colleagues observed of the Corman-Drosten iteration - whose designers apparently relied not on science but on social media science to inform assumptions about “it” being a SARS-related virus.
thanks; you write really well; and reaching out is to me great; I read others like Jamie Andrews, also doing great work; sad to see him rage over others in what I feel is his group; (ie maybe the V things don't exist): we at least need to let folks say that or discuss it; given all the freedoms we are meant to boast of; that our western world supposedly values so deeply
What is being called "animal viruses" might just turn out to be a lab artifact - something that doesn't exist outside the lab.
When the scientists are studying a sample of "a virus" in their test tube, the sample doesn't originate from an animal; the origin of "the virus" is ALWAYS from the chicken eggs, or from the cancer cells in the test tube or petri dish, used to generate "the virus".