
NYC's "COVID Only" Deaths in Spring 2020
Another sign that the Big Apple's big spike is specious

There is yet another data oddity related to the New York City spring 2020 death spike: a disproportionate number of deaths that list COVID-19 as the only cause of death.
Understanding the aberration, which I’ll show further into this article, requires a bit of background knowledge.
COVID-19 as the Sole Cause of Death
Contrary to popular belief, deaths that list COVID-19 as cause of death and nothing else are not “the only true COVID deaths.” They are deaths involving incomplete death certificates.
Robert Anderson, chief of mortality statistics at NCHS, provided a good explanation of this in a 12 March 2021 interview.1 (Ignore the problems with using a test result irrespective of symptoms to code a COVID-19 death - and the lack of evidence for a novel virus named SARS-CoV-2 causing a new disease - and focus on the death certificate completion aspect.)
HOST: For the death certificate, NCHS issued a guidance report – a guidance document – for certifiers on how to include COVID-19 on the death certificate. That came out about a year ago. Can you talk about that a little bit?
ROBERT ANDERSON: Sure. At the beginning of the pandemic, we realized that we had an opportunity to reach out to physicians to help them understand how to complete the death certificate – in general, not just with regard to COVID-19.2 And so we created this document that was specific to COVID-19 that showed them how to fill out the death certificate properly in general, and then once they determined that COVID-19 was either the cause of death or a contributing factor, how to report it on the death certificate. This guidance just sort of builds on guidance that we issued several years earlier – I think the last time we issued guidance, general guidance, was in 2003. This guidance is essentially the same – it’s just specific to COVID-19. This builds on the guidance that we issued before.
HOST: Turning to another topic here: comorbidities, other conditions contributing or involved with COVID-19 deaths. There was some confusion about the note on Table 3 on the website on COVID-19 deaths by contributing condition. The note says “For 6% of these deaths COVID-19 was the only cause mentioned on the death certificate.” And this has led to some wild and inaccurate speculation that the other 94% of the deaths may have been really some other cause of death and not COVID-19. Could you talk about that a little bit?
ROBERT ANDERSON: Yeah sure. I can provide a little bit of background here. The cause of death section on the death certificate is designed in a specific way and it’s designed to elicit a sequence of events leading to death. And then also to gather any significant conditions that contributed to death. So you have Part One about “cause of death” section which asks the certifier to provide the causal sequence. And so you would start on the top line and you would put the immediate cause of death.
To use a COVID-19 example, you might have “respiratory distress syndrome” which is a common complication of COVID-19. And then you would work backwards from that immediate cause of death. And let’s suppose that respiratory distress was brought on by pneumonia, viral pneumonia, and so you would put on the second line “viral pneumonia.” And then on the third line – because we want to know what the cause of viral pneumonia was – if it was COVID-19, then you would write COVID-19 on the third line. So you’d have respiratory distress due to viral pneumonia due to COVID-19. That’s a logical causal sequence from the immediate cause working back to the underlying cause. And then in Part Two, you could put any other conditions that might have contributed to death but weren’t part of that causal pathway in Part One.
Now with a disease like COVID-19, it should be fairly unusual to see only COVID-19 reported – I mean normally we should at least see the complications caused by the disease, such as pneumonia or respiratory distress. In cases where only COVID-19 is reported, the certifier is indicating that COVID-19 was the cause of death, but really they left it – the cause of death statement – somewhat incomplete. They neglected to provide the entire causal pathway.
Now with regard to the other 94% which mentioned other diseases or conditions, it’s important to understand that in the overwhelming majority of these cases the additional diseases or conditions are either complications of COVID-19 – they are in the causal pathway, like pneumonia or respiratory distress – or they’re reported in Part Two as contributing conditions.
So for about 92% of the deaths involving COVID-19 that mention other conditions –91 or 92% – the certifiers indicated that COVID-19 is the primary or underlying cause. This is not a situation where the certifier is writing all of the diseases that the person had equally; they’re actually reporting it in this causal sequence. And in the overwhelming majority of cases, COVID-19 has been indicated as the cause of the death. It’s the cause that started that causal pathway, that causal sequence leading to death.
The guidance Mr. Anderson is referring to includes examples of death certificates completed according to standards.3 He’s essentially saying death certificates for which COVID-19 is the only cause listed were not filled out correctly. The records are missing information about the link(s) between COVID-19, i.e., conditions it triggered or were that exacerbated by it and led to death.4
COVID-Only Deaths in the U.S. and New York City: March - May 2020
How many “COVID only” death records are there for the U.S. in spring 2020, and what proportion are from New York City?
Using a method confirmed by CDC staff, I queried the federal mortality database for such deaths in the U.S. and NYC, from March 1 (the day the first New York City case was announced) through May 31, 2020.
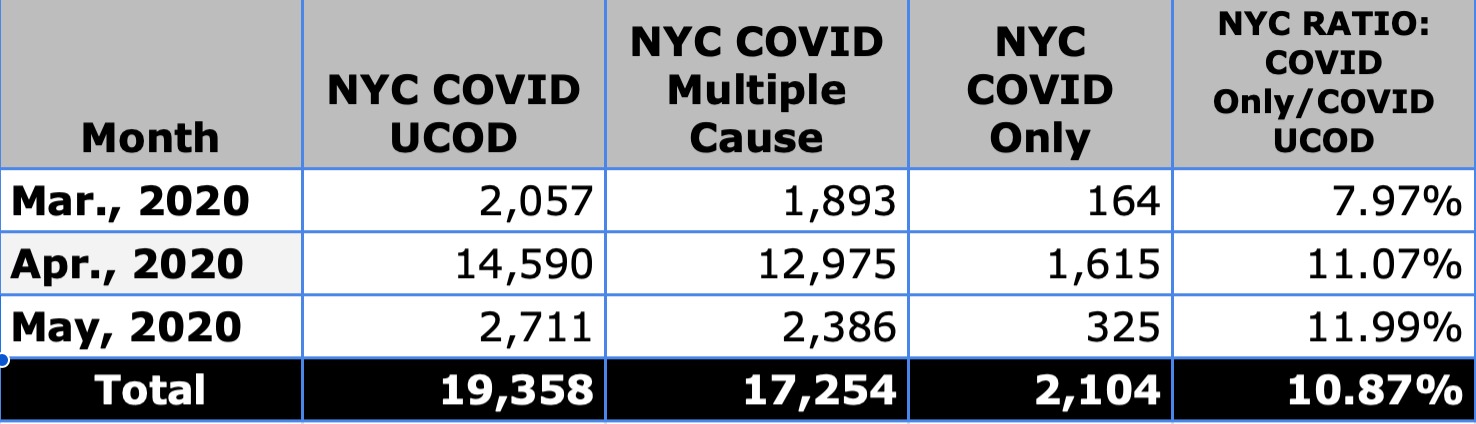
There were 103,797 deaths in the U.S. which list COVID-19 (U07.1) as underlying cause. Most list a “multiple” cause, - i.e., they are “complete” with respect to a documented causal pathway - while 7% incorrectly listed or entered only COVID-19. A lower rate is desirable; however, some level of error is understandable when a new cause of death/death code is announced out of the blue and doesn’t seem particularly unique from other respiratory illnesses or disease.

New York City’s ratios for the same timeframe are higher: Almost 11% of deaths with COVID as underlying cause list COVID as the only cause. Most of the COVID-only deaths (81%; n=1,715) occurred in hospitals, where one would expect coding procedures to be followed more closely than for deaths occurring at personal homes or nursing homes. Roughly a third are under age 65 (n=558/2,104)
The proportion of all COVID-related deaths that occurred in New York City in spring of 2020 relative to the U.S. is very high. Less than 3% of the population lives in one of the five boroughs, yet it’s where 19% of the country’s deaths with COVID listed as underlying cause occurred.
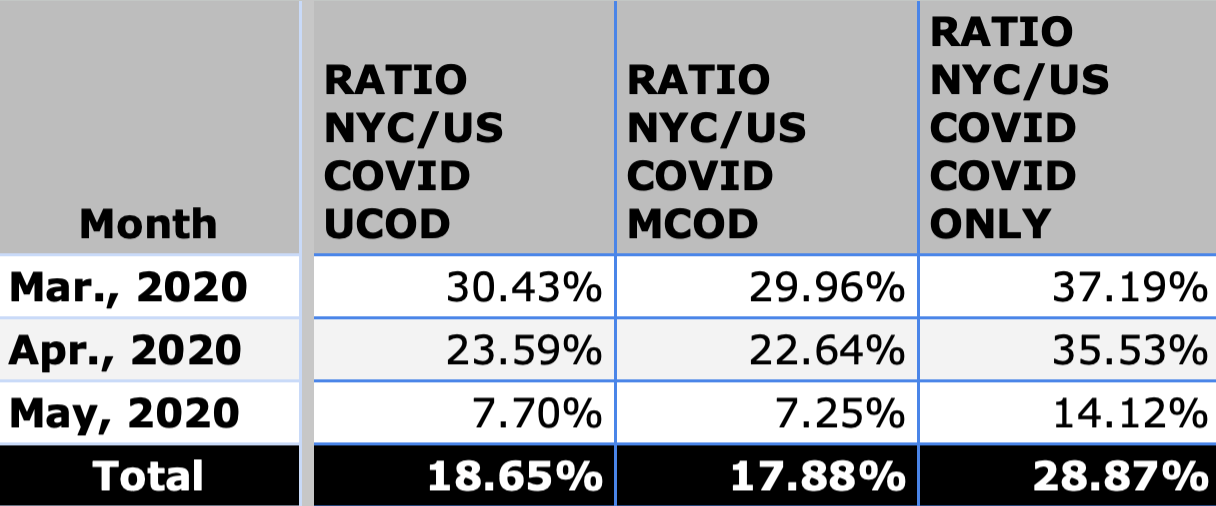
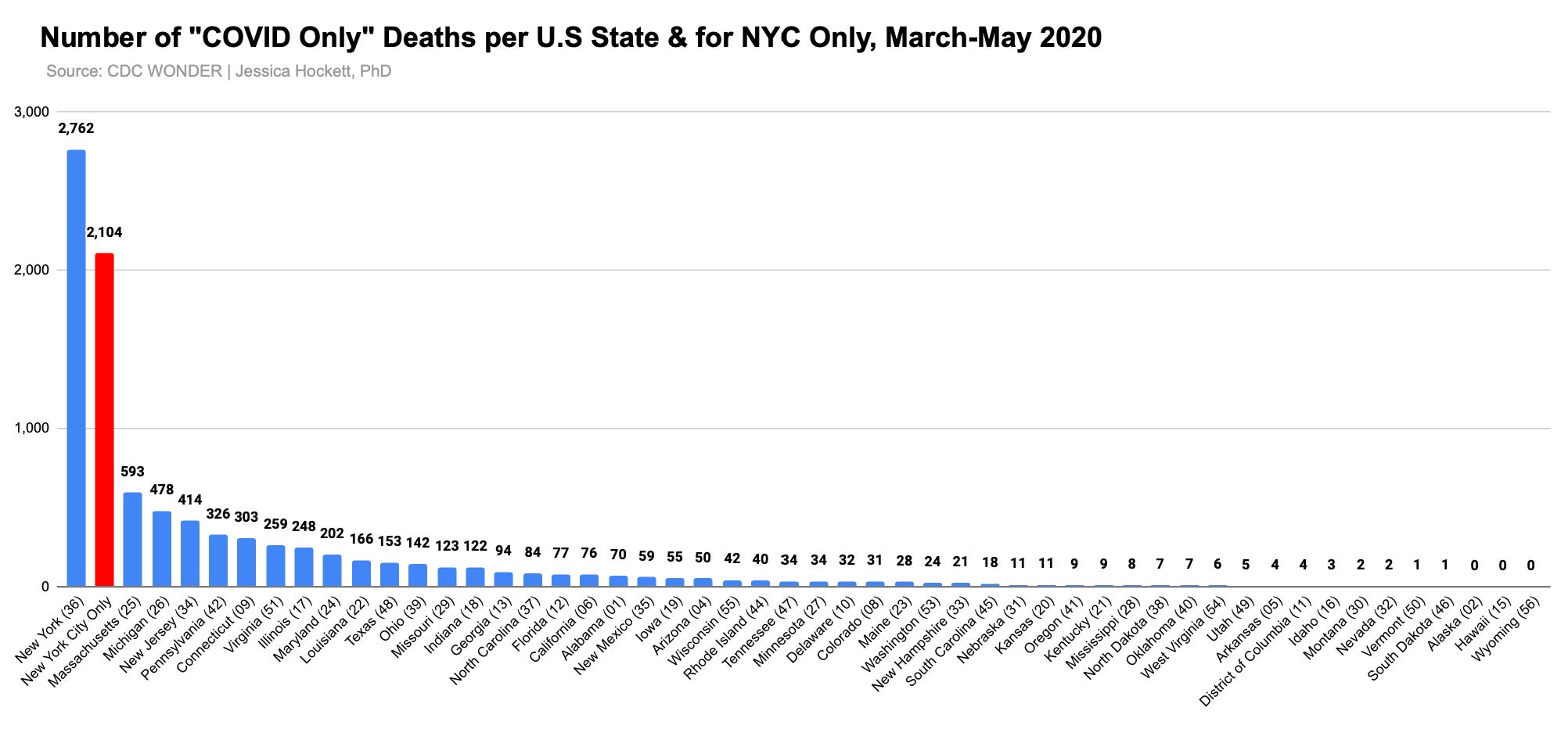
The ratio is higher for COVID-only deaths. Nearly 30% of such deaths in the first three months of the national emergency were in New York City — and more than a third in March and April.5
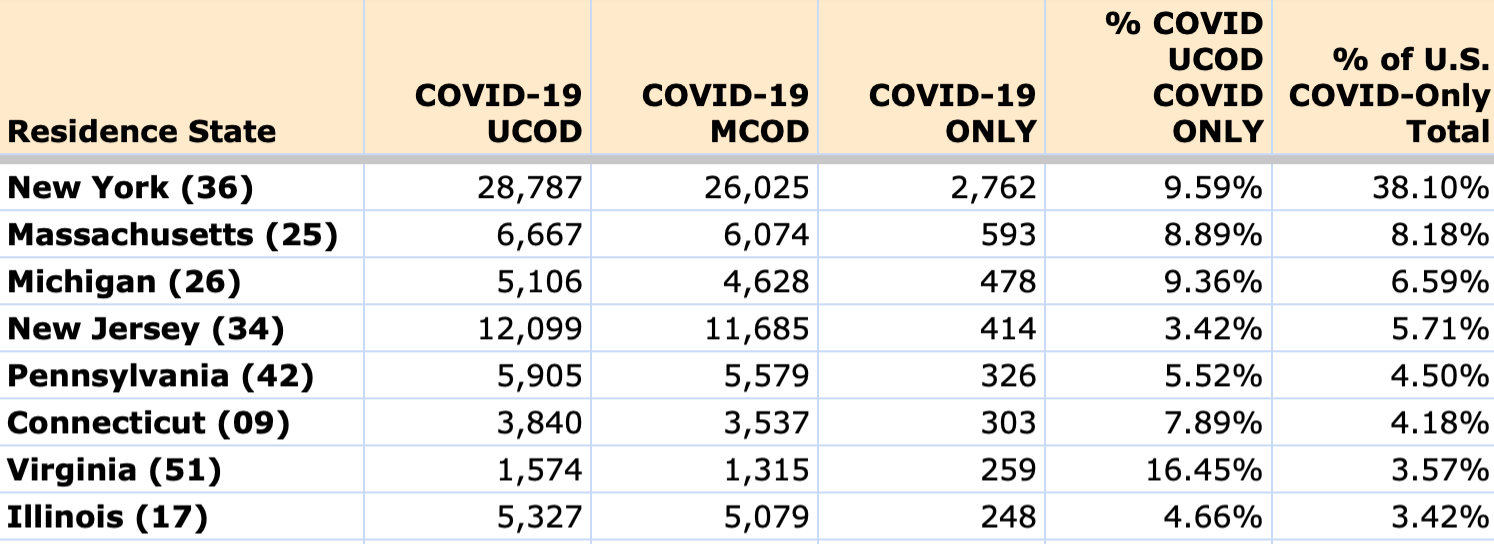
Outside of New York state, the counties that comprise the greatest portion of “wave 1” COVID-only deaths in the U.S. are in Massachusetts, Michigan, New Jersey, Pennsylvania, Connecticut, Virginia, and Illinois. None comes close to New York as a percentage of the U.S. total and NYC is 76% of the NY state total.
Expected or Unexpected?
Is the disproportionate number of NYC COVID-only deaths for spring 2020 in the U.S. total expected or unexpected?
On the “expected” side, it could be argued that COVID-19 (whatever it is) was operationalized and “reacted to” in New York City more vigorously than virtually anyplace else in America, which created stress and pressures inside hospitals that affected doctors’ abilities to follow new guidelines. The public hospitals auspiciously announced a full transition to the EPIC record-keeping system around the time CARES Act was passed and an executive order issued 23 March 2020 seems to relieve medical personnel of “requirements to maintain medical records that accurately reflect the evaluation and treatment of patients, or requirements to assign diagnostic codes or to create or maintain other records for billing purpose.”
On the “unexpected” side, because reasons like record-keeping & coding problems serve the government’s “New York got hit harder and was overwhelmed” narrative very well, such explanations should be regarded with suspicion. Federal coding guidance issued at the time was fairly clear, and it’s not easy to give NYC a pass when other cities didn’t seem to have the same kind of difficulty to the same extent.
For example, Cook County, Illinois (Chicago) reported the second-highest overall COVID death total in any single county in the U.S. for March-May 2020.6 Yet Cook reported 119 COVID-only deaths for those months out of 3,688 deaths that listed COVID as underlying cause (3%).7 Applying the 3% rate means New York City should have seen fewer than 600 COVID-only deaths, instead of more than 2,100. Had that been the case, the U.S. rate for COVID-only deaths in the spring would be closer to 5% instead of 7%.
It’s worth noting that the Cook County medical examiner’s work is automatically subject to public scrutiny in Cook County. We can see every death the ME processed, including those in a COVID deaths archive activated in March 2020. By contrast, the NYC Medical Examiner’s determinations are hidden, can’t be obtained by any citizen via freedom of information request, and the agency hasn’t been compelled to explain much of anything, including a data-processing event involving 11,000 deaths or a drop in autopsies conducted on deaths at home.8 Such lack of transparency appears intentional and makes it hard to see ultra-disaster-prepared New York City as an innocent bystander of a coronavirus attack that sent death-recording protocols to the bottom of the East River.
“COVID Only” - Not the Only New York Anomaly
If New York’s outsize proportion of COVID-only deaths were the only “anomaly” involved in its mass-casualty event, it could be chalked up to things like abrupt changes to hospital environments & record-keeping procedures, psychological warfare against healthcare workers, and/or confusing directives from administrators. But it’s one of many signals that something strange and thus far undisclosed occurred in a period that saw ~27,000 deaths.
While continuing to find curious patterns & discrepancies in the New York City death spike has put us past the point of being shocked by new findings, it doesn’t mean the high ratio of COVID-only deaths should be recused from interrogation.
Among the questions any thinking person should ask are
Who were the people whose deaths list only COVID? For those that died in hospitals, how did they get to the hospital, when were they admitted, and for what were they admitted?
Did some hospitals/hospital systems have more COVID-only death records than others?
Were the COVID-only deaths more likely or less likely to receive FEMA COVID-19 Funeral Assistance? Were they more likely or less likely to be buried on Hart Island?
What percentage of COVID-only deaths are linked to a positive test for SARS-CoV-2?9
Did cities/area in other countries that saw unusually-high death spikes - e.g., Lombardy, London, Madrid - also report a lot of COVID-only deaths, or is NYC again global outlier (like it appears to be with younger deaths)?
New York played a starring role in launching and substantiating a pandemic declaration and National Emergency decree. The fact that no one has been held accountable for or given sensical, data-aligned explanations for what happened there is deeply concerning. Whatever the factors that influenced the city’s COVID-only death toll, the public deserves an inquiry and full review of death records and patient charts.
Afterword (added 2 Sept 2024)
An article I wrote earlier this year - “The CDC Does Not Maintain Complete Death Certificate Collections” - is a good companion to the above analysis.

Key points:
In the U.S., deaths are registered at the state or local (county/city) level.
Many states record deaths electronically and do not automatically generate or provide death certificates (as PDFs/paper copies).
Local jurisdictions/states do not submit death certificates to the NVSS, NCHS, CDC or other federal entity — they submit death certificate/death data.
The federal government seems to believe that electronic death registration systems (EDRS) are necessarily less prone to error, completion issues, etc. I disagree and contend that the kinds of accuracy issues may change but EDRS’s have their own issues and may make it easier for data to be manipulated, including remotely or by federal agencies.
The federal government (NCHS/NVSS/CDC) position seems to be that virtual records in every state should be confidential. I disagree and contend that, in most cases, birth, marriage, and death records should be public insofar as the recording of the events involving individuals is concerned. The fact that Vincenza Abbate died at age 57 in Brooklyn, New York, on October 17, 1918 is not a private matter. Public agencies are stewards of the records; they do not own them apart from We the People and should not be able to privatize them.
All of this is important to keep in mind when evaluating the NYC death spike event and “COVID-Only” anomaly. Electronic systems and digital death data make fraud and intentionally-uncorrected errors very feasible. Unlike Denis Rancourt and others, I do not accept without reservation that all-cause death curves are impervious to bias and should be accepted as necessarily true in the absence of public records that show individual decedents. It only takes one manipulated curve in one city to render the curve of a whole country false.
(Added 4 Sept 2024)
The city’s 2020 Vital Statistics report includes a special section on COVID-19 mortality with an explanation for differences in COVID death numbers previously used by the city health department and those in the final report. Page 66 says:
With the beginning of the COVID-19 pandemic, the NYC Health Department implemented several measures to ensure complete ascertainment of COVID-19 deaths, as adequate nosology guidance did not exist, doctors did not necessarily know how to complete the cause of death section on the death certificate, and testing for the disease was extremely limited. To ensure the best possible ascertainment, the team worked very closely with the NYC DOHMH ICS/Surveillance Epidemiology team to monitor cases, including matching lab records of COVID-19 tests with the death registry. This allowed real-time reporting of COVID-19 deaths in a time when total deaths were increasing rapidly.
Guidance did exist and testing was not limited, especially in hospitals.
What is meant by a team “matching lab records of COVID-19 tests with the death registry” is unclear. “Real-time death reporting” regardless of cause is near-impossible and the whole paragraph is an apologetic/defense for changes to COVID death numbers. Although the report doesn’t mention deaths that list COVID-19 as the only cause, claims that doctors didn’t know what they were doing because they weren’t given proper directions is probably what officials would say if pressed about the COVID-only death entries.
h/t @PalerRider1980 for making me aware of this transcript
Per Understanding Death Data Quality: Cause of Death from Death Certificates, an estimated 20-30% of U.S. death certifications have completeness issues (e.g., missing information, incorrect completion of causal pathway, misidentified place of death). This doesn’t necessarily or always create inaccurate death certificates but it can affect the quality of information.
Some of the documents, examples, and training modules Mr. Anderson mentions can be found at Reporting and Coding Deaths Due to COVID-19. Several models for death certificate completion can also be accessed directly here.
National Vital Statistics System alert regarding the new code was issued on 24 March 2020, after the American Hospital Association (AHA) sent a request to Secretary of State Azar to immediately implement unique ICD codes for COVID-19 disease, exposure to COVID-19 and screening for the virus. See 31 Jan 2020 and 18 March 2020 entries in this timeline for additional info on the WHO creating the ICD code and the decisions to activate it sooner than originally planned.
For comparison, I requested COVID-only death data from the NYC bureau of vital statistics. The numbers for March - May 2020 are comparable to those in the federal database. Seventy percent of the year’s COVID-only deaths occurred in April, the same month most deaths listing COVID as the only cause occurred.
Chicago is America’s third most-populous city and is demographically-comparable to New York. The difference in magnitude between New York’s and Chicago’s daily all-cause death curves in spring 2020 is considerable. Alongside Bergamo (another event that - like New York - appears to involve Democide and data manipulation), the trio paint a portrait of absurd (if implicit) assertions that are impossible to explain as the work of a spreading coronavirus.
CDC WONDER
FYI: NYC Chief Medical Examiner Dr. Barbara Sampson served in the role from 2013-2021 and presided over controversial cause of death determinations for Joan Rivers & Jeffrey Epstein and had worked at OCME during the September 11, 2001 World Trade Center disaster. Cleary Dr. Sampson was an experienced government official who could be relied upon by superiors in high-profile and crisis situations.
Early guidance gave a fairly wide berth to doctors/medical examiners, et al insofar as putting COVID-19 on a death certificate without record of a positive test. For example, the 24 March 2020 bulletin says: “Should ‘COVID-19’ be reported on the death certificate only with a confirmed test? COVID-19 should be reported on the death certificate for all decedents where the disease caused or is assumed to have caused or contributed to death. Certifiers should include as much detail as possible based on their knowledge of the case, medical records, laboratory testing, etc. If the decedent had other chronic conditions such as COPD or asthma that may have also contributed, these conditions can be reported in Part II.”
When comparing NYCity to NYState Co-Morbidity List, during the real-time reporting on their Java Tracker page of Deaths, 10 comobies were listed. NYState strangely omitted OBESITY. This skews the Covid-only deaths to the upside yet your chart shows a lower overall NYS C_O % than NYC's. Maybe they revised their list.
I think this is one of your best pieces, Jessica. This is very impressive research and citizen journalism. You continue to ask questions no one else is asking and the dots you are connecting ... don't connect, according to the "official narrative." ... And you're still not getting all the "public" information, you've requested.
To me, the fact they made it easier to assign a death to "Covid only" by - again - "changing the guidance" - should be (and is) very significant info.
P.S. Regarding the death certificate guidance changes, stay tuned to my Substack.