One COVID-related misconception repeated by Americans since 2020 goes something like this:
The CDC’s own data say only 5% of COVID deaths in the U.S. don’t list comorbidities — these are the only “real” COVID deaths!!!
The CDC lies about a lot of things. In this case, however, the idea that U.S. deaths listing COVID-19 as the sole cause of death represent “the only real COVID deaths” distorts what the agency has actually said.
Here, I review the CDC’s official explanation for such deaths, recap why I consider the number and proportion of “COVID-only” deaths during the New York City mass-casualty event a fraud signal, and comment on recently reported “COVID-only” deaths elsewhere.
“COVID Only”: What the CDC Says — and Says it Means
Per U.S. standards established by the National Center for Health Statistics (NCHS), a death certificate designates one underlying cause of death, followed by conditions that describe the causal sequence leading to death.1
There’s technically no fixed limit to how many contributing causes may be entered, though most electronic death registration systems (EDRS) that states use accommodate roughly 20–25 causes in total, including the underlying cause.2
COVID-19 as underlying and sole cause of death
Since the advent of its Provisional Death Counts and COVID-19 page (now archived), the CDC has reported that a certain percentage, typically around 5-6%, of U.S. death certificates that list COVID-19 (U07.1) as the underlying cause also list COVID-19 as the only cause of death.
One reason that people began misinterpreting this statistic might be due to how it is phrased under Table 3 on the page: “Comorbidities and other conditions”:3
The number of deaths that mention one or more of the conditions indicated is shown for all deaths involving COVID-19 and by age groups. For over 5% of these deaths, COVID-19 was the only cause mentioned on the death certificate.
Responding to a question about this phrasing on a CDC podcast in March 2021, chief of mortality statistics Dr. Robert Anderson explained:
[W]ith a disease like COVID-19, it should be fairly unusual to see only COVID-19 reported – I mean normally we should at least see the complications caused by the disease, such as pneumonia or respiratory distress. In cases where only COVID-19 is reported, the certifier is indicating that COVID-19 was the cause of death, but really they left it – the cause of death statement – somewhat incomplete. They neglected to provide the entire causal pathway.
Now with regard to the other 94% which mentioned other diseases or conditions, it’s important to understand that in the overwhelming majority of these cases the additional diseases or conditions are either complications of COVID-19 – they are in the causal pathway, like pneumonia or respiratory distress – or they’re reported in Part Two as contributing conditions.
Anderson helped write the guidelines for COVID-19 death certification, which do make clear that a death listing COVID-19 as the underlying cause should include at least one contributing condition establishing a plausible causal chain.4
From March through May 2020, 103,797 deaths in the U.S. listed COVID-19 (U07.1) as underlying cause. About 7% of those list no other cause besides COVID-19.5
Can this figure be called “fairly unusual” as Anderson put it? Perhaps not, given the sudden rollout of new coding rules for an ostensibly novel disease that was indistinguishable from existing illnesses and conditions.
New York City’s “COVID-Only” Ratio
My continuing interest in COVID-only deaths is rooted in the spring 2020 New York City mass-fatality event, which shows higher ratios of such deaths than the national pattern.
During March–May 2020, nearly 11% of NYC deaths listing COVID-19 as underlying cause also listed it as the only cause, which is roughly 50 percent above the U.S. average. Even more anomalous: 81% of those “COVID-only” deaths (n = 1,715) occurred in hospitals, where one would expect the highest accuracy in certification.
Roughly one-third of these were deaths under age 65 (n=558 of 2,104). Younger-adult COVID deaths in hospitals are one of many anomalies about the New York event. Official data claiming, in effect, that a significant portion say COVID-19 was the only cause of death is another red flag.
Less than 3 percent of Americans live in one of New York City’s five boroughs, yet in spring 2020 the city accounted for 19 percent of all U.S. deaths listing COVID-19 as underlying or contributing cause. For “COVID-only” deaths, the imbalance was even starker: nearly 30% of such deaths nationwide in the first three months of the emergency occurred in NYC, and more than a third in March and April 2020.
Outside the five boroughs, the counties with the largest “wave 1” COVID-only totals were in Massachusetts, Michigan, New Jersey, Pennsylvania, Connecticut, Virginia, and Illinois, but none came close to New York’s share. Within the New York state, New York City alone accounted for 76% of all “COVID-only” deaths.
For the data above and further discussion of whether concentration of “COVID-only” deaths in New York City is a reason to suspect fraud, see “NYC’s COVID-Only Deaths in Spring 2020”.
Beyond the U.S.
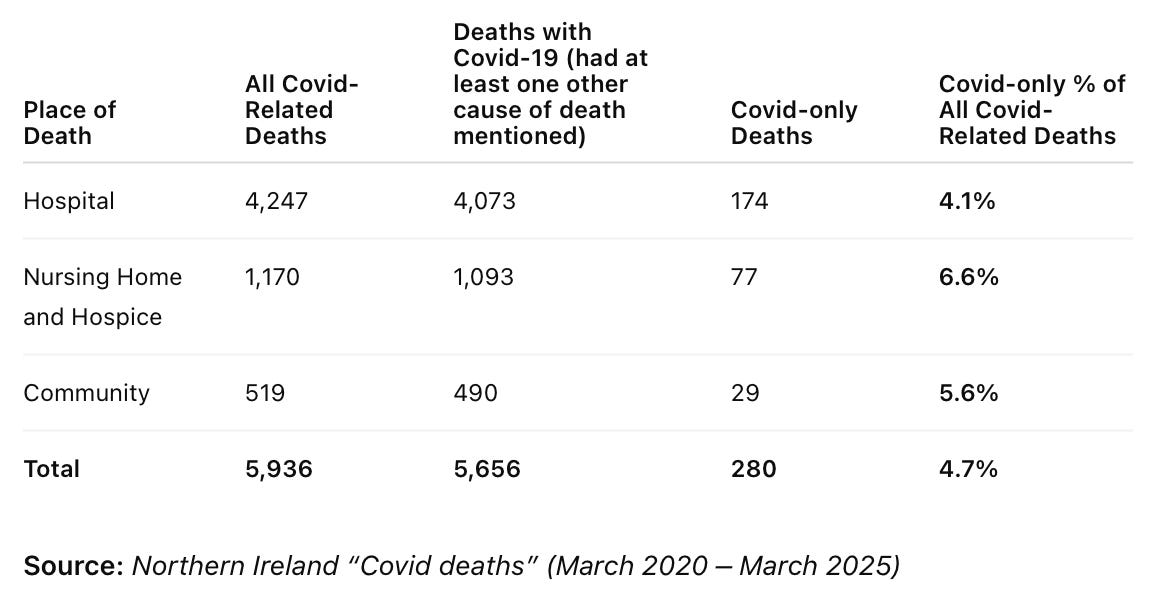
The “COVID-only” question isn’t unique to the United States. A recent article by Norman Fenton, Kathy Grey, and Martin Neil highlighted the presence of (what they termed) “COVID-alone” deaths in Northern Ireland data obtained through a freedom of information request.
Because of what the CDC has said explicitly about the designation, I interpret the low cumulative proportion of such deaths to all deaths with COVID on the death certification (4.7%, comparable to the U.S.) as an artifact of new coding guidance and sloppiness on the part of whomever recorded the death. Fenton et al use the data to make a different point about the number of influenza-attributed deaths versus COVID only deaths; an official explanation from the relevant authoritative body would be useful for international comparison.
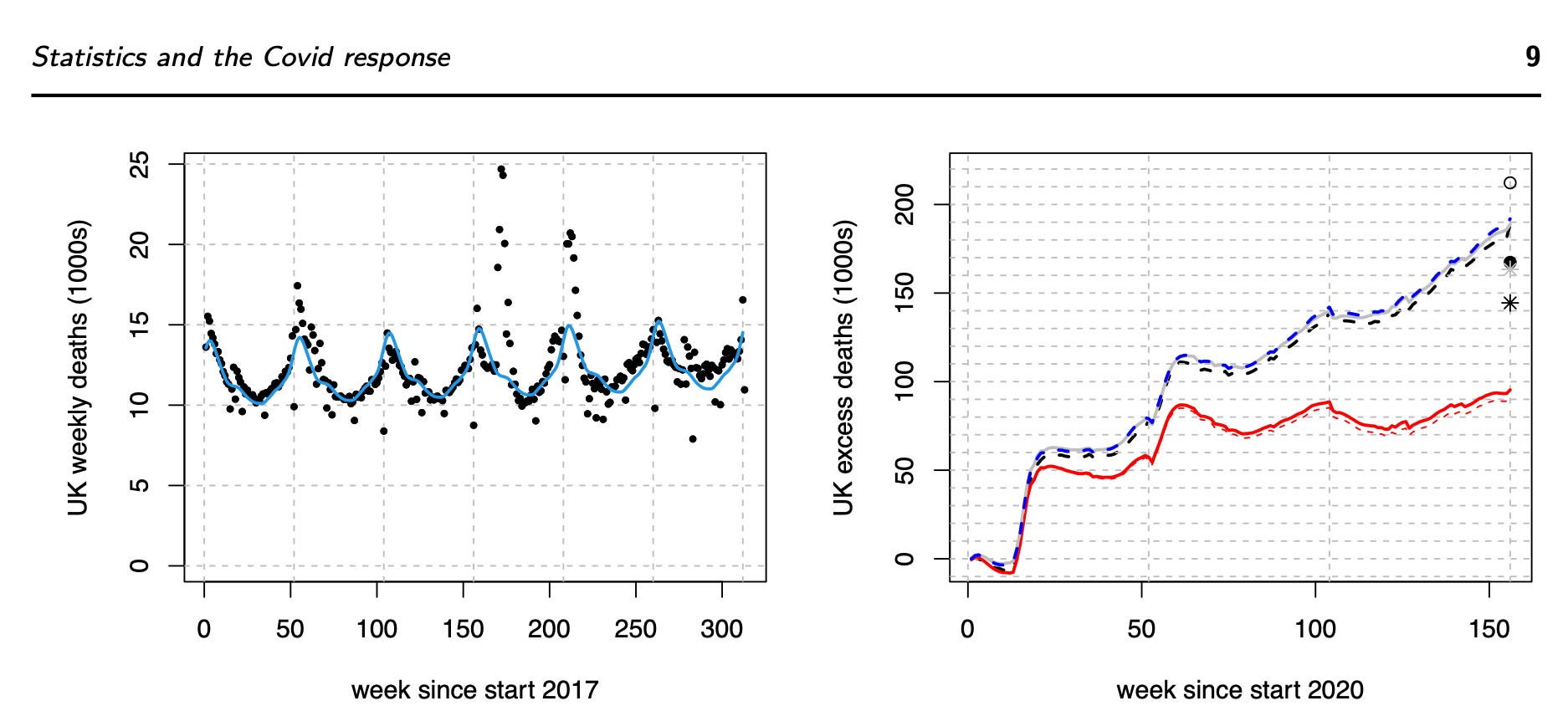
A paper presented to the Royal Statistical Society in April 2025 and recently accepted for publication — “Some Statistical Aspects of the COVID-19 Response”by Dr. Simon Wood of the University of Edinburgh and colleagues — analyzes UKdata on cumulative excess deaths between March 2020 and December 2022 and mentions Covid only deaths: [emphasis mine]
The cumulative excess deaths shown in red in the right panel of figure 4 are much lower than the total deaths recorded with Covid (212,247 with Covid mentioned on the death certificate by the end of 2022, according to the UK government’s data dashboard). There are a number of mechanisms that are likely to account for this.
An obvious one is the fact that only some 17 thousand people had only Covid and nothing else recorded on their death certificate. When Covid is only one factor among several in a death, it is statistically naive to expect it to contribute a whole extra death in the excess figures (given that some of the other factors are risks contributing to what is expected without Covid).
Put slightly more technically, since dying with Covid and dying with other co-morbidities are not independent events, Covid mortality events do not simply add to the mortality caused by the other co-morbidities. Related to this are what epidemiologists refer to as ‘harvesting’ effects where an epidemic pathogen brings forward the deaths of some very frail people by only a few weeks or months. Over a period of three years many such people will not appear as excess deaths at all, since their death has only been moved within the time period considered.
Wood et al are saying measured excess deaths — how many more people died than expected, per a model — are far fewer than the total number of deaths officially recorded as “with Covid” (i.e., Covid is listed somewhere on the death record). The difference, they say, suggests that many deaths labeled as COVID weren’t additive and didn’t actually add to the overall mortality count. Statistically, the deaths replaced or overlapped with deaths that would have happened anyway.
Even within the paradigm that accepts COVID-19 as a unique disease, unless we know how UK agencies (e.g., NHS, UKHSA, ONS) regard a death that lists COVID as the sole cause, it’s not possible to treat the 8% (17,000 of 212,247) either as ‘pure’ or ‘true’ COVID deaths (so to speak), or see them as people unlikely to have died were it not for a new thing called COVID, which is what Wood and colleagues seem to imply.
I emailed Simon Wood on 21 September 2025:
Good afternoon, Dr. Wood.
My name is Jessica Hockett. I’m an independent researcher of the COVID Event from the United States. I’ve investigated the New York City mass-casualty event of spring 2020 and — to a lesser extent — the Lombardy/Bergamo event that preceded it.
In your accepted manuscript you wrote that “only some 17 thousand people had only Covid and nothing else recorded on their death certificate.” I’ve analyzed the “COVID-only” designation as applied in New York City compared with the rest of the U.S. and would be glad to share that analysis.
My question: Have you encountered—or are you aware of—any similar explanation or policy from U.K. authorities regarding “COVID-only” certificates?
Warm regards, Jessica Hockett, PhD
I have not received a reply.
Though Wood et al don’t challenge the WHO’s claim that COVID-19 was a novel spreading disease caused by a SARS-related virus, they might at least concede that presence and incidence of “COVID alone” deaths in all countries casts doubt on the official story about sudden onset of an illness that we are expected to believe temporarily shut out deaths normally attributed to influenza and other viruses, and therefore warrants closer scrutiny.
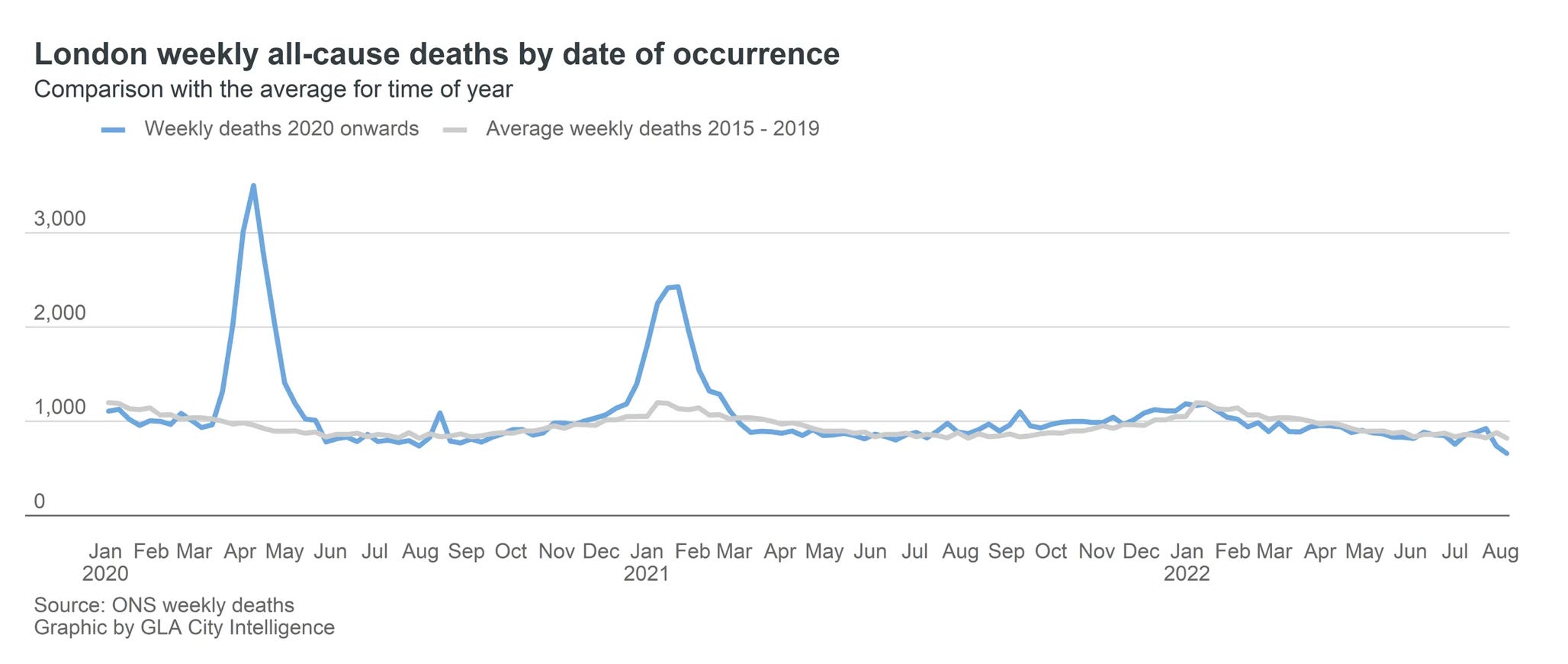
Given the audacity of London’s spring 2020 death curve, it seems important to know how many and what proportion of the 17,000 “only Covid” deaths occurred there and in what settings.
A Very Good Place to Start
For now, Americans, at least, should resist the claim that “COVID-only” deaths reveal some “truth” about the illness or deaths associated with it, because federal health agencies apparently regard such death certificates as incomplete. Whether that explanation can be trusted, given how much and how often those same agencies have deceived the public over the past five years, is another matter.
Authorities in all countries should be compelled to clarify how they interpret death records that list COVID as the sole cause, in light of local or national guidance published for doctors and medical examiners. A relatively high number or proportion of “COVID-only” deaths in a location should not be regarded as evidence the area was suddenly struck by a deadly new pathogen but an anomaly demanding investigation.
On that front, New York City remains a very good place to start.
“Let’s start at the very beginning…a very good place to start…”
For more on CDC WONDER multiple cause database, see this overview from Mary Pat Campbell. My understanding is that underlying cause is usually what actuarial analyses involve and is of highest interest to insurance companies.
On a personal note, I remember using the comorbidity data on this page in 2020 and 2021 to show that COVID-19 apparently killed those who were very much on the edge and already in poor health.
I haven’t delved into recent and historical patterns or trends among U.S. death certificates listing only one underlying case — regardless of what it is — and no contributing causes, but Anderson seems to suggest that such cases would also be classified as incomplete. I inquired with life actuary and WONDER “wizard” Mary Pat Campbell, who signaled interest in the question and may be able to provide an answer.