
The F Word
What I mean when I say I believe the New York City 2020 death curve is fraudulent

Last year,
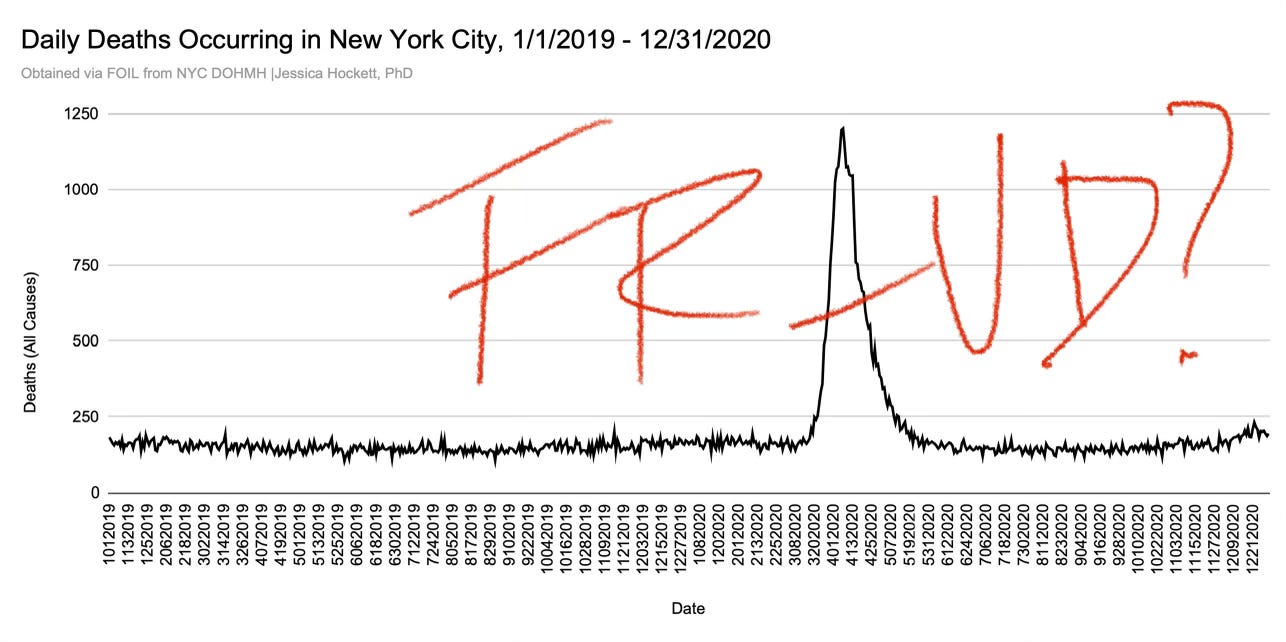
colleagues & I questioned the veracity of New York City’s 2020 all-cause death curve and gave eight reasons for suspecting it might be false. We said the data “is incongruent with itself” but made no claims to being able to prove the numbers incorrect, nor did we assert that fraud took place.I’ve said many times that I personally believe the official New York City data are fraudulent. For the sake of clarity, and to document my thinking about the concept in one place, I explain here what I mean when I use “The F Word” with respect to the New York City event.
I am not (yet) presenting a complete argument using circumstantial evidence to show all of the fraud signals I see, or fully explaining all reasons why I think the curve is fraudulent, or defending the number of deaths I suspect are fraudulent.
Rather, I am expounding in general terms what I mean by a fraudulent or manipulated curve, speculating about the motive(s) for fraud, and mentioning or footnoting some of the examples that I’ve written or spoken about previously or plan to write more about in the future.
What is Fraud?
Every sensible definition of the word “fraud” involves misrepresentation with intent to deceive.
Unlike legitimate errors or mistakes, fraud doesn’t just “happen.” There is no “Whoops, I committed fraud.”
One or more individuals has to do something that shouldn’t be done, or not do something that should be done, legally-, ethically-, or morally-speaking.
The motive for fraud usually involves financial, professional, or personal gain. There could also be a desire or need to protect self or others from losing power, credibility, stature, or opportunity. (Readers can hearken myriad examples, I’m sure. Elizabeth Holmes and the Theranos endeavor come to my mind, as do a number of Illinois politicians.)

Fraud involving COVID-19 as a New Cause of Death vs All-Cause Death Fraud
Discussions about death fraud per se in the COVID Era are typically focused on a) whether there was a new cause of death, i.e., COVID-19, and b) the extent to which deaths have been accurately attributed to that new cause, versus to another cause.
Lying about a new cause of death or publishing guidelines which tell doctors & coroners to falsely attribute a cause of death is certainly an act of fraud. Generous counting strategies freely disclosed in press conferences in spring 2020 were always concerning and continue to be so.1
However, when I say the New York City death curve is fraudulent, I’m not chiefly referring to whether someone died “from or with” COVID, or to whether a newly-detected/freshly-named virus caused any deaths at all.
I’m saying there is no proof that the number of people who are purported to have died on each day in New York City
actually died on the days claimed,
died in the setting/places they are said to have died, and
died only once (i.e., the deaths is recorded only once in all city, state, and federal records).
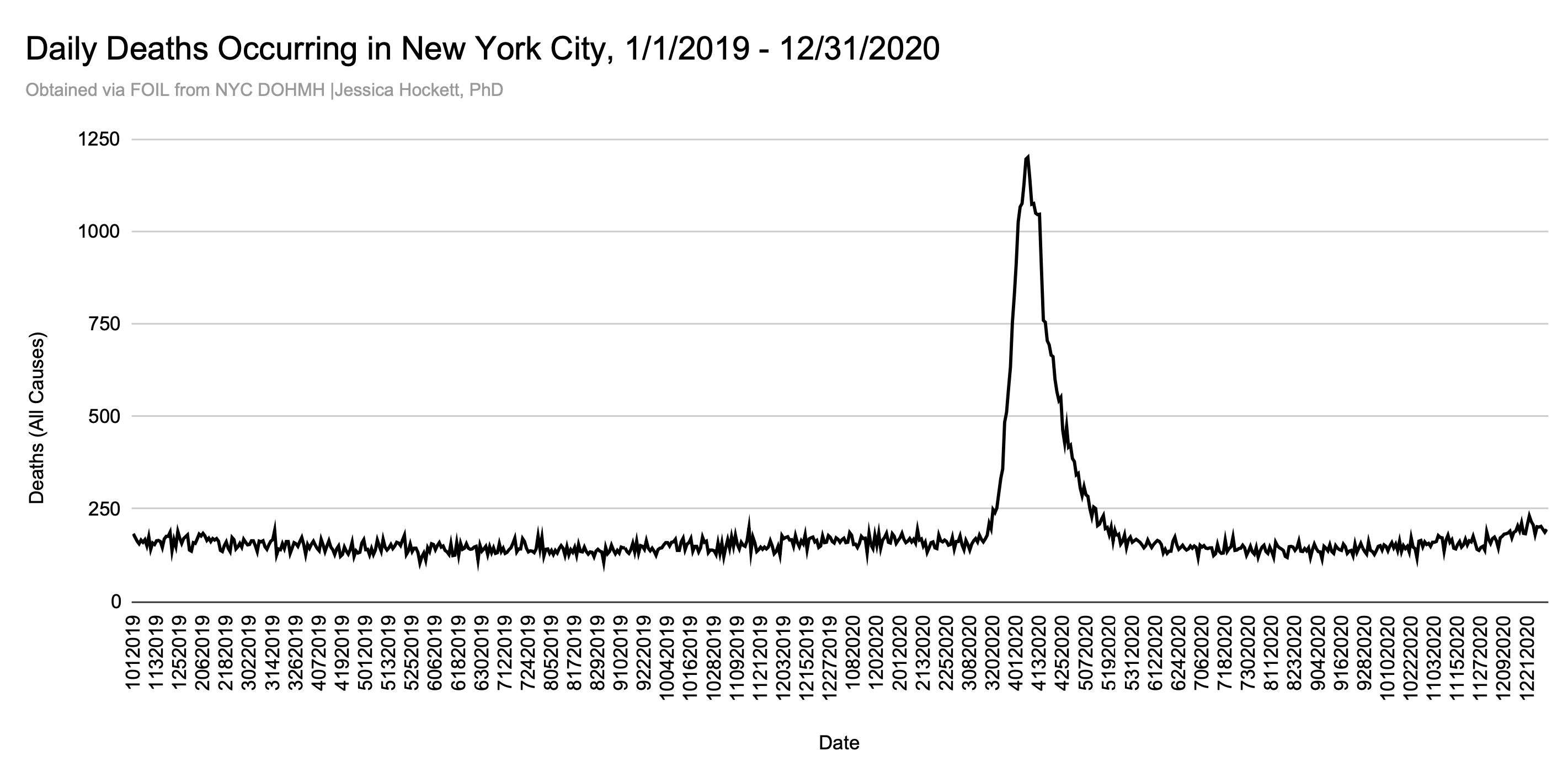
Officials at all levels of government have failed to substantiate the spring 2020 event with any kind of basic proof (e.g., a complete list of names, death certificates, an archive of the medical examiners determinations). For that reason and many others, it is my current opinion that New York City’s all-cause death curve and multiple underlying & associated curves do not depict a real-time death event — regardless of what caused the deaths.
If the New York event didn’t happen as presented by official data, then it’s a fraudulent or manipulated curve, because it does not reflect what happened “on the ground” on those days.
Six Kinds of Fraud (What a Fraudulent Death Curve Could Include or Involve)
A fraudulent curve is not synonymous with faked deaths. There are six kinds of death fraud I propose could be involved in contriving or manufacturing the magnitude, timing, and/or trajectory of deaths in New York City for 2020. These types are not exhaustive, nor are they mutually exclusive.2
1. Made-Up/Fabricated Deaths
Made-Up or Fabricated Deaths would involve death certificates that aren’t attached to decedents (“phantom deaths”) and/or numbers that can’t be corroborated by death certificates.
Generating death records for people who never existed or “fudging the numbers” by adding or subtracting digits are fairly easy feats to accomplish, if risky in the long-run, because future legislation, lawsuits, executive orders, or a formal inquiry could compel the deaths records to be released to the public.
However, given the battles that groups like Reclaim the Records have faced in getting New York City to release decades-old death certificates, there’s a good chance anyone involved in faking deaths would be dead by the time someone forces the release of 2020 death certificates.
Simple examples of facts that lend credence to the idea that some of the deaths could be faked follow:
There were 2,233 New York City resident deaths in 2020 that listed COVID-19 - and only COVID-19 - as cause of death3 Contrary to popular belief, death certificates which list COVID-19 (U07.1) as underlying cause with no other contributing causes listed are not “the only real COVID-19 deaths.” They are incomplete death certificates. The fact that over 10% of deaths which list COVID-19 as underlying cause are incomplete death certificates is a red flag.4
Due to the World Trade Center disaster in 2001, the New York City Office of the Medical Examiner (OCME) had considerable experience with issuing death certificates in the absence of a body.5 Such a task makes sense with the nature of the event and difficulty of recovering & identifying human remains. If the spring 2020 event was presented to the OCME as very fast, this prior experience could have been leveraged for fabricating deaths.
While fabricated deaths have never been my primary contention, the sheer audacity of the curve’s magnitude & speed (the rise and the fall) is enough to set-off anyone’s “BS” detector.6 Without a list of names, or a way of getting death certificates, I have to allow for the possibility that some portion of the death toll could have been faked.
2. Moved Deaths
Moved Deaths are deaths that would have occurred at some point before or after the excess mortality event (i.e., mid-March thru the end of May 2020), possibly not recorded or processed, and either “pushed forward” into the future or “pulled back” into the past to help create or augment the Main Event spike.
Moved Deaths could also be deaths that occurred in another state or jurisdiction, and/or among non-NYC residents, that were recorded as having occurred in New York City and/or among NYC residents.
3. Held-Back Deaths
Held-Back Deaths are similar to Moved Deaths, but involve intentionally delaying the processing of deaths or “storing them up” in anticipation of “needing” them at an appointed time. Such storage could be digital or physical - as in holding bodies in storage.
If more deaths than normal are occurring, but you don’t want the public to know until a certain time, digitally withholding the deaths from processing for weeks or months would be.a fairly easy thing to do.
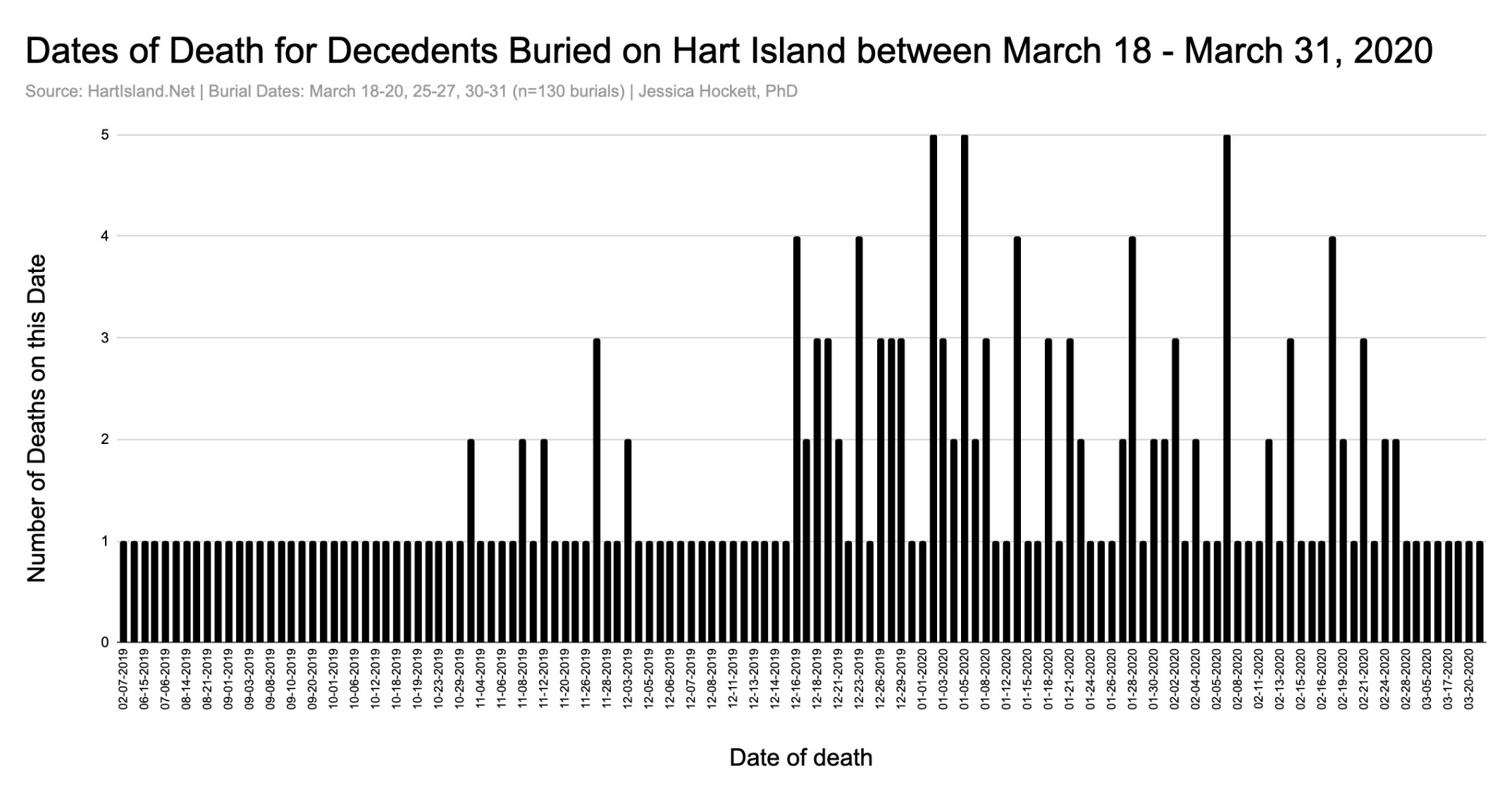
Holding bodies in storage may sound like an episode fromThe Sopranos, but it isn’t necessarily a departure from what’s normal in New York City. The city has a public-burial site - Hart Island - for unclaimed decedents and those who elect a city burial for themselves or a loved one. By definition, unclaimed decedents have been in storage for some period of time.
Data scraped from HartIsland.net shows that many months can pass before decedents are buried.7 For example, only seven of 200 decedents buried on Hart Island in the latter half of March 2020 were people who died in March. Half (n=100) had died in 2019.8
4. Reclassified/Stolen Deaths.
Reclassified or “Stolen” Deaths are also similar to Moved Deaths, but refer to deaths that would have occurred in the distant past (6+ months or longer) and were recorded with certain or unknown causes and fully processed.
A fraud operation would reach back, “steal” the deaths from the past (with or without the corresponding statistics or reports being adjusted), and then reclassify the deaths in one or more ways (e.g., as COVID-19 deaths).
This possibility is especially plausible if COVID-19 has alternate or additional meaning(s). For example, if it also means Covert/Coordinated Operation for Vaccine-Induced Disease, then deaths occurring because of or associated with another shot (e.g., flu shots) could be reclassified under “COVID-19.”
5. Double-Counted Deaths.
Double-Counted Deaths are deaths that occurred during or close to the 11-week event but are counted more than once. For example:
Deaths that occurred in one place/setting of death but counted in another place of death as well, i.e., New York City residents who died at Home being counted in the Hospital death total and Home death total.
Deaths that occurred in a different county but are also counted as occurring in one of the five counties that comprise NYC. One can imagine “confusion” over city versus state deaths due to the shared name (New York) .9
6. Displaced Deaths
As a form of fraud, Displaced Deaths aren’t as much related to the all-cause death curve as they are to the underlying place of death curves and totals, because they involve an intentional change to where people would normally be expected to die.
I see at least two possibilities along these lines:
Digital changes that moved some or many deaths which occurred in one place of death to other places of death - without double-counting. For example, counting some hospice facility deaths as hospital inpatient deaths.10
Putting measures in place that could cause even the normal number of deaths that would occur (not only excess deaths) to occur elsewhere. An example of this would be sending critically ill/on-the-edge nursing home and/or hospice facility patients into the hospital, testing them for Novel Virus before they’re sent or upon arrival, and allowing them to die there or expediting their deaths via protocols.11 (Such a strategy would also have the advantage of leading doctors & nurses to believe a sudden-spreading illness was overtaking the city and help explain some of the patterns in clinical observations that some “frontline” workers have described.)
All of the Above? Some of the Above? None of the Above?
The six forms of death fraud I’ve described are not exhaustive. They are possibilities I’ve induced from comparing different datasets of many kinds (i.e., not only death data) and from reviewing contemporaneous reports & subsequent actions taken (or not taken) by officials.
While the six techniques are "equal” in terms of the skills, tools, or collusion that would be required to “pull off” successfully, I’m not proposing anything I consider impossible. No doubt intelligence agencies, the military, and Silicon Valley have the ability to create any number of death illusions.12
If death-data fraud is involved in the New York City event, I doubt there is only one kind of fraud. A complex, well-designed operation would involve multiple layers of obfuscation - some that could be readily or easily explained in the future as “errors.”
A government-assisted/-encouraged propaganda campaign could very easily steer media coverage toward reporting things in real-time which can be blamed later, in the event that public pressure, whistleblowers, or a lawsuit threaten full exposure.
Examples of such Potential Future Excuses (my term) I’ve derived from reports during and subsequent to the New York City event follow:
There were too many changes to coding guidance!
We didn’t have enough staff!
The guys from FEMA did that counting!
We were switching to a new a patient record system!
Our systems were overwhelmed!
New York the state, not New York the city!
The dashboard said so!
They weren’t counting COVID deaths at home!
The National Guard took care of that part!
We meant probable deaths, not probable COVID deaths!13
Any plan worth its salt (including an ex post facto cover-up strategy) would of course include “safety valves” that aim to ensure no single thing could be blamed or expose everything that happened in one fell swoop.
Impetus for Fraud
Why would the New York City death curve be (or need to be) manipulated at all?
It’s hard to deny that without the New York City event, there would have been no selling Americans - or the rest of the world - on the WHO Pandemic Declaration or the story of a *Novel Spreading Virus in Need of New Treatments and a Dedicated Shot.*
No “Live from New York!” Pandemic Show? No chance people would’ve believed a deadly coronavirus was on the loose. As
put it so brilliantly to me once,“You don’t launch a pandemic from Provo, Utah. It’s gotta be New York.”
He’s right.
Thanks to Hollywood, New York has been seared into our collective consciousness as a City Under Attack. Real-life attacks, like the World Trade Center disaster in September 2001, help reinforce the image of the Big Apple perpetually facing Big Risks. New York is also the media capital of the world, home to the United Nations, and (arguably) the most disaster-prepared city in the United States. Few places are more iconic of freedom and democracy — or more used to being center stage.14
New York is also population-dense. This matters, because no one is going to believe a Spreading Deadly Virus is either spreading or deadly if it doesn’t appear to spread and kill people in a city where people live close together. Unless the New Thing does New and Bad Things in New York, people will question the need to “lock down,” test, use new or repurposed treatments, and warp-speed a shot.
All of that to say, “NEW-YORK-CITY-GOT-ATTACKED-BY-A-CORONAVIRUS” is a story in need of protection. Would people in power commit fraud to seed, sow, and keep selling the story? Of course they would.
I believe any fraud is premeditated, but I could also envision a scenario where the ScaryModels flashed on screens as Harbingers of Doom set a bar that couldn’t be reached. Allow me to explain:
Despite what public officials, the CNN news crawler, & Johns Hopkins University implied, real-time death reporting isn’t possible, simply due to how deaths are processed.15 It’s possible various dashboards were too generous in their real-time reporting, and there was a genuine “Uh oh” moment on the part of officials when reality wasn’t able to keep up with or “realize” the models’ predictions. Rather than admit an error, steps were taken to cover it up by manipulating data to make deaths - and possibly other data like ambulance dispatches - “fit” the event which models had fed into reporting systems.
I’m speculating, of course, but given the lack of transparency about All Things COVID, such a scenario is hardly the stuff of a wild imagination.
It’s worth noting that March 2020 wasn’t the first time death projections for a pandemic in New York City had been made. Anticipated deaths for an eight-week pandemic flu event can be found in the New York City medical examiner’s office “Pandemic Influenza Surge Plan for Managing In- and Out-of-Hospital Deaths” published in 2008.16 The plan anticipated at least one “outbreak” wave resulting in a single large-scale mass fatality event with potential subsequent waves.
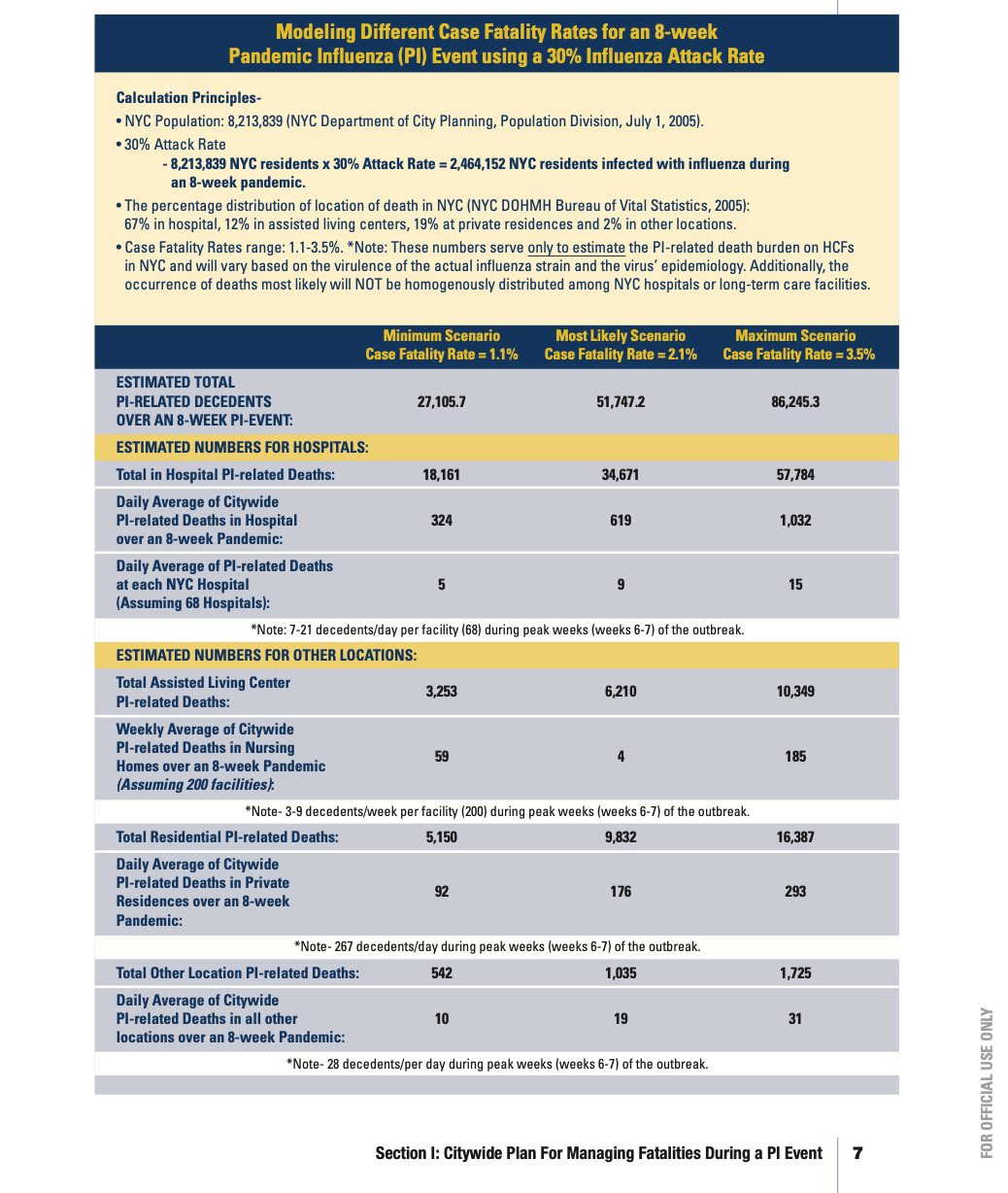
Three estimates of Case Fatality Rates based on models were proposed. The “Minimum Scenario” estimated 27,106 pneumonia & influenza (P&I)-related deaths in eight weeks.17 This number is very close to the number Andrew Cuomo shouted at a press conference and (more importantly) to the actual reported increase in the excess period.18
Whether this estimate was a “goal” is hard to say, but the 2008 surge plan provides a basis beyond mere conjecture to wonder if there was a target. If the target was going to be reached no matter what - or if the target was “missed” due to something failing to go as planned - a fraud effort involving things like moving or fabricating deaths seems highly plausible.19
To be clear, I am not saying New York City experienced no excess death in the spring of 2020. I’m sure it did. But, in my opinion, it did not occur at the magnitude or speed which official data claim, nor in the timeframe alleged.20
We Need Proof
None of the six techniques for committing all-cause death fraud outlined above is failsafe. Criminals - even very smart ones - always make mistakes. Whether those mistakes are caught and proven is another matter altogether.
If the New York City 2020 daily death curve is manipulated in any way, it presents a serious challenge to the WHO pandemic declaration, the U.S. government’s endorsement thereof, and everything that followed. It would also give reasons to question death curves in other cities around the world. After all, like the song says, “if you can make it there, you can make it anywhere.”
We need proof America’s largest city experienced such an extreme and sudden loss of life. Without proof, the possibility of fraud can’t be dismissed.
Please send any data, factual, and/or typo corrections to WoodHouseSub@proton.me
Two examples are responses from Deborah Birx and Illinois Department of Public Health director Ngozi Ezike on April 7, 2020 and April 19, 2020, respectively, who each said that people who tested positive for COVID-19 and died are considered COVID-19 deaths, regardless of other causes or conditions. This approach was unethical for many reasons, but was consistent with WHO guidelines.
The terms I am using are my own. They are not derived from another source, and I am not suggesting that professional auditors or mortality experts would use such terms.
Data obtained via freedom of information request. Request submitted on November 14, 2023 and received on February 26, 2024.
According to data provided to me by NYC DOHMH, there were 21,439 deaths that occurred New York City in 2020 which attributed COVID-19 as underlying cause.
See page 50 in the NYC DOHMH 2001 Vital Statistics Report
The conclusion of a statistically-adept friend who has analyzed some of the data from the New York event is "Jessica, they just made that s*** up.”
h/t @gishgallop for assistance with the database
New York City “coronavirus deaths” listed inThe New York Times “Incalculable Loss” feature on May 24, 2020 are underrepresented as a proportion of total COVID-19 deaths. I find this interesting and a potential indicator that double-counting could’ve occurred on the data side.
A March 23, 2020 executive order issued by Governor Andrew Cuomo allowed Subdivision (2-b) of Section 4002 of the Public Health Law to be suspended or modified “to the extent necessary to allow a hospice residence to designate any number of beds within such facility as dually certified inpatient bed.” The 13% drop in deaths occurring in hospice facilities raises the question of whether a portion of the hospital inpatient death toll includes hospice facility patients who were in “dually certified” inpatient beds.
This is a reason I requested data on daily ambulance transfers from nursing homes to hospitals on March 2, 2023. I’m still waiting on the Fire Department of New York City (FDNY) to provide those records.
It wouldn’t surprise me if some had been done on a smaller scale for other purposes in years past - either as practice or for “national security” reasons.
On April 14, 2020, New York City announced the addition of ~3,700 “probable” COVID deaths to its toll. The deaths had allegedly occurred between March 11th and April 13th. By June 1, probable COVID deaths totaled 4,516, per the CDC’s outbreak report for New York City. These deaths have been an ongoing source of suspicion and examination for me and warrant discussion in a separate article. See The COVID Death Reckoning and the “Deaths in the Mass Casualty Event that Were Blamed” section in my Very Long Letter to Will Jones for my previous observations about the probable COVID deaths.
A later version may exist that I haven’t yet been able to locate or obtain.
I rounded up from 27,105.7 because there is no such thing as a .7 death.
Between 26,000-27,000 depending on source (NYC DOHMH vs. CDC WONDER)
All three estimates in the Office of the Medical Examiner’s 2008 surge plan strike me as incredibly high for disease-spread event over an eight-week period. On page 6, the authors explain several assumptions and expert uncertainty around such an event: National planning experts have not been able to characterize fully how a PI event might unfold. PI deaths will likely increase and decrease in waves, over a 12 -18 month period nationally, affecting NYC for several weeks. Many agencies use a 5 -7% mortality rate of the infected population (as indicated by the Department of Defense Joint Task Force Civil Support), but vary the time period when these fatalities may occur. Some experts believe a PI event may encompass two or three 8-week periods, spanned over 8 -10 months.” Archival news articles gathered by Mark Kulacz suggest that, over time, the U.S. government, WHO, et al have increased their estimates of Spanish flu deaths. Like 2020, the 1918 event involves numerous iatrogenic factors. It’s possible that estimates used by pandemic/bioterrorism preparedness efforts have modeled an impossible respiratory illness event. For this and other reasons, I agree with Mark that the 1918 narrative needs to be corrected.
Thank you for pressing this issue. My assumption is that the NYC death curve originated from a model. The authorities were not going to chance reality canceling their pandemic program.
If the death curve of 2020-2021 is suspect then the post Covid-19 2024 deaths must also be suspect.