
False Binaries that 'Limit the Spectrum of Acceptable Opinion' in the COVID-19 Debate and Perpetuate Lies Told by The Powers That Be (Part 2)



The technique of infamy is to start two lies at once and get people arguing heatedly over which is the truth. (often attributed to Ezra Pound)
Part 1 of this series argued for the existence of ‘false binaries' that have steered the public away from questioning the WHO’s claims about a transmitting viral threat.

Binaries—also known as dichotomies or forced dilemmas—are powerful persuasive tools because they reduce complex issues to simple opposites: affirmative/negative, yea/nay, for/against. The goal isn’t necessarily to prove one position absolutely true and the other absolutely false, but rather to set out two, and only two, opposing views so that people begin to think differently and some broader objective is achieved, such as victory, consensus, or resolution.
A false binary, however, is a logical fallacy that limits debate by denying that other perspectives exist (or pretending they don't) and, by doing so, manipulates, misleads, or distorts the truth by suppressing or failing to acknowledge valid alternatives. This is precisely what governments and media did with all things COVID: promote limited possibilities, permit certain kinds of dissent, and suppress or silence views that are most threatening to their narrative.
Central False Binary
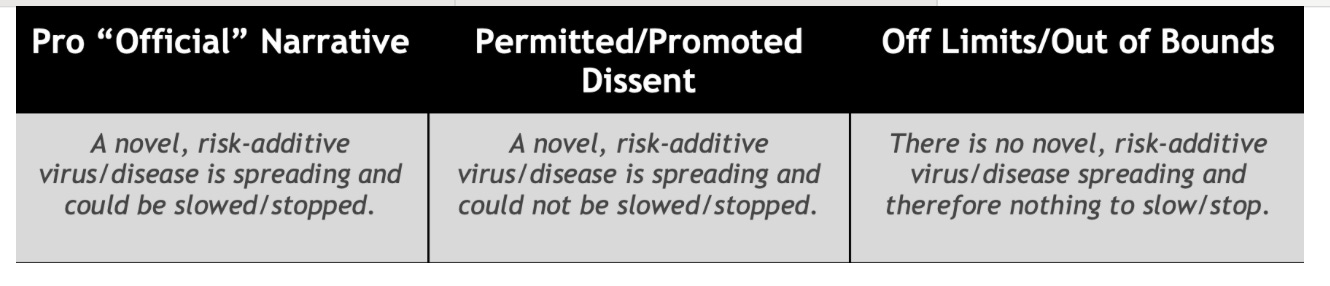
The central false binary proffered in the COVID event—and promulgated to this day — involves the claim a novel, risk-additive virus/disease was spreading, constituted a threat, and warranted a response of some kind. In March and April 2020, little to no “anti-lockdown” sentiment was afforded airtime or modeled by those in authority. Citizens were either COVID supporters or COVID deniers—“all in” for being safe, or “all alone” and being selfish.
On the Pro “Official” Narrative end of the spectrum was the idea that spread could be slowed or stopped. On the Permitted/Promoted Dissent end was the notion that spread could not be stopped or slowed but the most vulnerable could and should be protected from “it” for a time, until the "danger had passed" or until herd immunity was reached. The idea of there being no novel, risk-additive virus or disease and therefore nothing to spread or stop—and focused protection inhumane regardless—was (and still is) Off Limits/Out of Bounds.
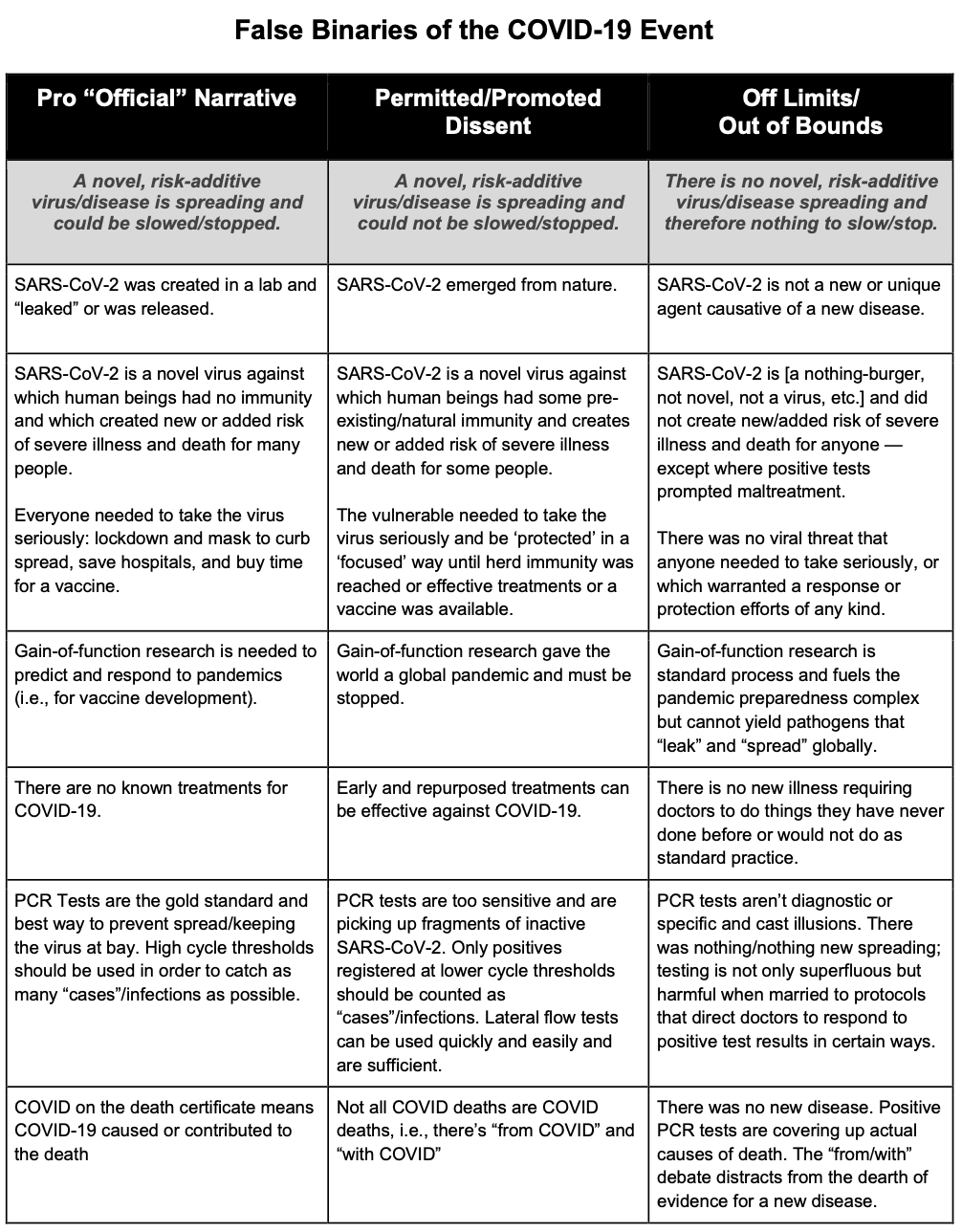
The constituent parts of the views illustrated above can be dissected further:
Pro Narrative: SARS-CoV-2 is a novel virus against which human beings had no immunity and which created new or added risk of severe illness and death for many people. Everyone needed to take the virus seriously: lockdown and mask to curb spread, save hospitals, and buy time for a vaccine.
Permitted Dissent: SARS-CoV-2 is a novel virus against which human beings had some pre-existing/natural immunity and creates new/added risk of severe illness and death for some people. The vulnerable needed to take the virus seriously and be ‘protected’ in a ‘focused’ way until herd immunity was reached or effective treatments or vaccine was available.
Off Limits: SARS-CoV-2 is a nothing-burger, not novel, not a virus, etc., and did not create new/added risk of severe illness and death for anyone—except where positive tests prompted maltreatment. There was no viral threat that anyone needed to take seriously or which warranted a response or protection efforts of any kind.
Supporting False Binaries: Strategic and Emergent
Numerous false binaries support the central false binary and are critical to preserving it. Some appear highly strategic, if not planted. Others are better described as emergent, with both “sides” not immediately evident and the controversies only developing after the initial months of “the emergency”.
Origins
The most prolific and persistent supporting false binary regards the ‘origin’ of SARS-CoV-2; namely, whether “it” leaked from a lab or came from a wet market or other zoonotic incident. These scenarios were planted in January 2020 and soldier on, with few signs of allowing for other possibilities anytime soon.

In the United States, the Pro Narrative and Permitted Dissent views on ‘origin’ have now switched places, with officials, media, and self-interested parties continuing to protect the public from perspectives that fall Out of Bounds. Views such as viruses don’t exist; SARS-CoV-2 is a non-spreading computer construct; the coronavirus was novel to detection but had been circulating for years; and COVID-19 is not caused by a SARS virus imperil the veracity of claims inherent in emergency decrees about emergent and manmade pathogens, as well as preparedness efforts for future pandemics.
An associated false binary involves the once and future role of gain-of-function research.
Pro Narrative: Gain-of-function research is needed to predict and respond to pandemics (i.e., for vaccine development).
Permitted Dissent: Gain-of-function research gave the world a global pandemic and must be stopped.
Out-of-Bounds: Gain-of-function research is standard process and fuels the pandemic preparedness complex but cannot yield pathogens that “leak” and “spread” globally.1
After a high-profile, orchestrated battle, the Pro-Narrative and Permitted Dissent sides are now unified, with recent actions taken by the U.S. sending the message we need safe gain-of-function research in order to combat the dangerous gain-of-function research that gave the world a pandemic.
Treatment
Another false binary that looks to have been strategically launched in 2020 was No Known Treatments versus Known/EarlyTreatments. The Pro-Narrative view, illustrated by statements from the WHO, was that there was “no known effective antiviral treatment” for the coronavirus.

The idea of early treatment for the novel virus was seeded early—consistent with the belief that antivirals for flu are effective only if taken “early” in illness. A February 2020 Lancet study by Chinese researchers endorsed “early detection, early diagnosis, early isolation, and early treatment.”2 What became Permitted Dissent centered on experimental and repurposed use of remdesivir and chloroquine/hydroxychloroquine, followed by protocols from individual doctors, new physician coalitions, and, later, an emphasis on Ivermectin.3
Yet No Known Treatments and Known/Early Treatments shared a core assumption: this was a new disease, not flu, requiring different interventions. What remained Off-Limits was the view that no new illness existed—nothing requiring doctors to do things they’d never done before or would not do as standard practice. That view is still unacknowledged by officials, researchers, and mainstream media.
If ventilators can be considered a “treatment,” their promotion as a weapon in the war on the virus was well underway by late February 2020 and reached a fever pitch during the New York City event. Elevated doctors and nurses featured in mainstream and social media didn’t reject the ventilator narrative outright—they promoted modified use without departing from or challenging the premise of a novel disease. Though the battle cry faded after “wave 1,” ventilators continued to be used widely and data for “COVID patients” on ventilators in ICUs reported.
Testing
A series of false binaries related to testing for SARS-CoV-2 emerged over the course of the ‘pandemic’ as well.
Given how central testing was to SARS-1 (2003), H1N1 (2009), and flu surveillance in the years leading up to 2020, the early push for widespread testing could not have been accidental. Massive numbers had to be tested for the newly-named entity to appear as if it were spreading. Immediate and substantial investments toward testing infrastructure advanced the Pro-Narrative claim that more testing would help “slow the spread”. Permitted Dissent urged testing only the symptomatic.4 The view that no testing was necessary at all remained strictly Off-Limits.
Another misleading dichotomy involved the sensitivity of PCR testing.5
Pro Narrative: PCR Tests are the gold standard and best way to prevent spread and keep the virus at bay. High cycle thresholds should be used in order to catch as many “cases”/infections as possible.
Permitted Dissent: PCR tests are too sensitive and are picking up fragments of inactive SARS-CoV-2. Only positives registered at lower cycle thresholds should be counted as “cases”/infections. Lateral flow tests can be used quickly and easily and are sufficient.
Off-Limits: PCR tests aren’t diagnostic or specific and cast illusions. There was nothing/nothing new spreading; testing is not only superfluous but harmful when married to protocols that direct doctors to respond to positive test results in certain ways.
The onset of mass testing for SARS-CoV-2 and advent of COVID-Like Illness (CLI) as a surveillance variable in March 2020 truncated the influenza surveillance season. When positive tests remained low to non-existent in many places, a false binary around flu ensued:
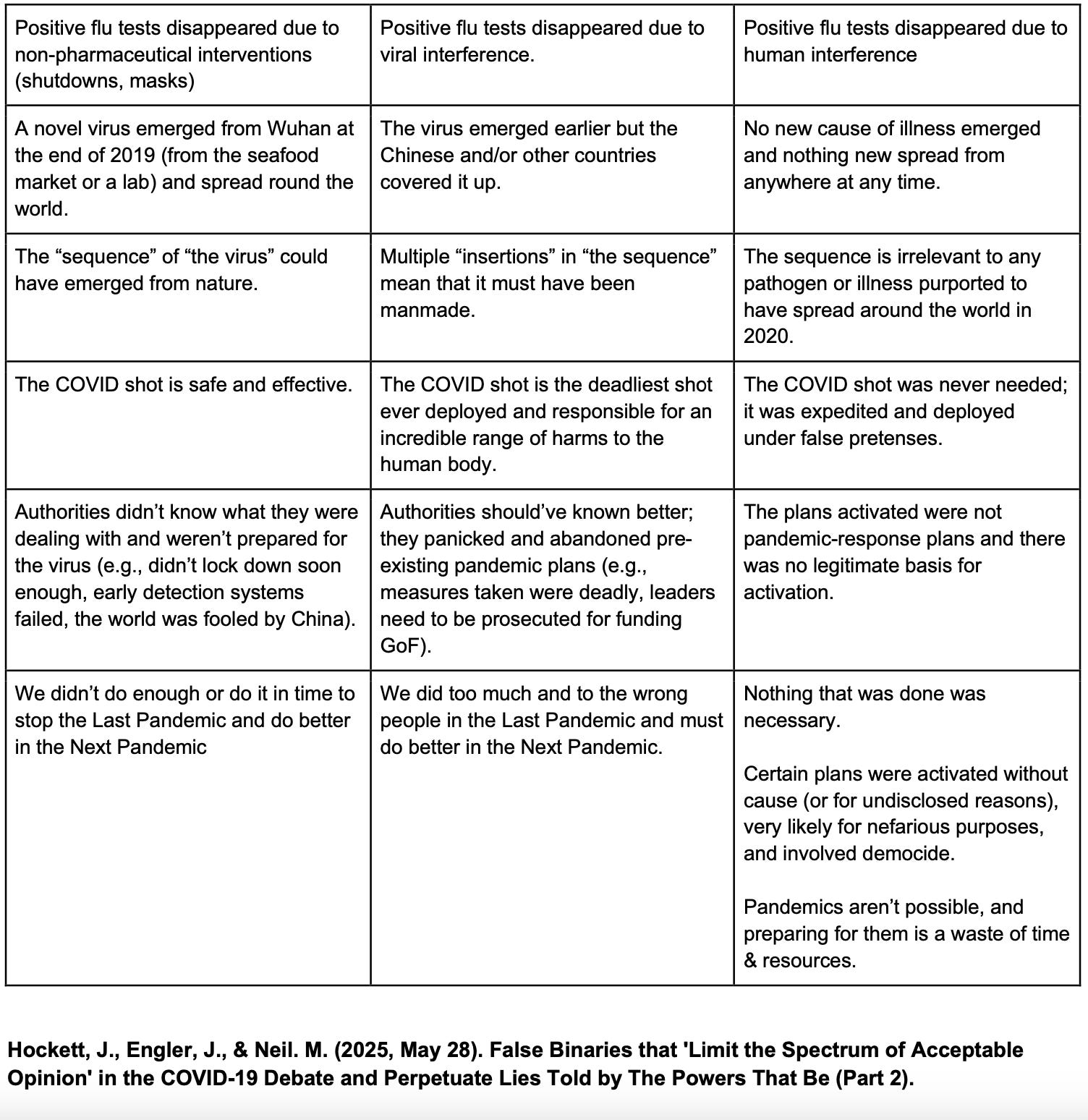
Pro Narrative: Positive flu tests disappeared due to non-pharmaceutical interventions (shutdowns, masks).
Permitted Dissent: Positive flu tests disappeared due to viral interference.
Off-Limits: Positive flu tests disappeared due to human interference.
From COVID/with COVID
Owing largely to a test-centric “case” definition and coding directives, a high number of deaths were immediately attributed to COVID-19. Statements by public officials quickly ignited the “from/with” debate.
In the U.S., for example, on April 7, 2020 and April 19, 2020, respectively, Deborah Birx and Illinois Department of Public Health director Ngozi Ezike each said that anyone who tested positive for COVID-19 and died would be counted as a COVID-19 death—regardless of other causes or conditions. While this approach raised ethical questions, it aligned with WHO guidelines.
Pro-Narrative voices insisted that, aside from a few cases involving non-natural causes, COVID-19 listed on a death certificate meant the associate virus or disease caused or contributed to death. Permitted Dissent countered that not all COVID deaths were truly COVID deaths—hence, the distinction between dying from COVID and with it. Some jurisdictions eventually began reporting “from/with” COVID hospitalization data.
A recent study from Greece, published in Nature, has been touted as vindication for the “from/with” perspective, but ultimately serves to reinforce the Narrative and deflects questions about what SARS-CoV-2 is, whether it causes respiratory illness, etc.
The idea that positive PCR tests have always obscured true causes of death—and that the “from/with” COVID debate distracts from the dearth of evidence for a new disease—remains firmly Out-of-Bounds.
“Start” of spread
A false binary related to “spread” has been promulgated by testing and a focus on specific events.
The Pro Narrative rendition is that a novel coronavirus emerged from in China toward the end of 2019 - whether at a seafood market or a lab. Theories involving a viral agent escaping or being “released” earlier in 2019, and/or from a lab other than the Wuhan Institute of Virology, with the responsible country or countries covering up what happened, appears to have been Permitted Dissent. Scrutiny of the World Military Games also falls within the bounds of what can be discussed with respect to the “beginning” of spread.
Out of Bounds, however, is the idea that no new cause of illness actually emerged or spread from anywhere at any time. Rather, the illusion was manufactured through PCR and antigen testing, seroprevalence studies, wastewater surveillance, and “retro-testing” of stored samples—with every bit of it promoted and legitimized by incessant waves of coordinated propaganda.
Meaning of “the sequence”
Much debate has transpired over what “the sequence” associated with SARS-CoV-2 truly represents. The Pro Narrative portrayal started by arguing that the sequence could and did arise naturally. Any suggestion that its various “insertions” prove “the virus” was manmade in a lab was the preserve of the Permitted Dissent camp.
Now those positions appear to have flipped, accompanied by great fanfare along the lines that “the mainstream media finally admits the truth”. We view this volte face as a deliberate, artificial move designed to distract people from a far more likely possibility—namely, the “the sequence” is an in silico construct with no relevance or causal link to illness observed in the real-world, and no capacity to spread from person-to-person around the globe. This and similar views remain firmly Out of Bounds.6
COVID Shot
A more controversial false binary to consider involves the COVID shot.
The Pro Narrative perspective, of course, was that the COVID shot is safe and effective (or mostly safe and effective).
Permitted Dissent has taken many forms, with the most extreme being that the COVID shot is the deadliest product ever deployed and is responsible for an incredible (and nearly impossible) range of harms to the human body. As with Origins and Gain-of-Function research, it could be argued that versions of the Permitted Dissent position have become—or are becoming—the dominant narrative.
Still Out-of-Bounds is the view that no one needed the COVID shot; it was expedited and deployed under false pretenses. Other angles on the shot are so marginal they defy easy classification and may not directly threaten the “sudden-spreading coronavirus” narrative but could be seen as a barrier to getting the COVID shot pulled from the market. Theories involving differential batches, data fraud, and psycho-social influences on the propensity to report averse events are still off limits.
Getting “unstuck”
Intentional or not, COVID debates became “trapped” within boundaries The Powers That Be deemed acceptable and non-threatening to their official pandemic story.
Noam Chomsky’s observation has proven correct: “Strictly limiting the spectrum of debate” while allowing or even encouraging certain critical views—so long as they don’t threaten the core lies—is “the smart way to keep people passive and obedient.”7
Which is why it’s important to recognize that, in some (though not all) circles, the conversation remains “stuck” as leaders and agencies continue issuing a steady stream of limited hangouts.
False binaries are blinding. Beneficial binaries, by contrast, are eye-opening and help surface nuance and reveal distinctions along a continuum. For example, There was a pandemic vs. There was no pandemic and A response to something was needed in 2020 vs. No response of any kind was needed.
The issue isn’t binary framing per se, but whether fundamental, obvious questions are being asked and addressed. No single, monolithic “resistance” to the WHO’s COVID narrative exists, after all, and the views of the average dissident are rarely black-and-white.8
Still, there is troubling alignment between the Pro-Narrative (“Covidian”) stance and many who consider themselves ‘Dissident” on the matter of whether a pandemic occurred. Disagreements tend to revolve around how much was done, when, and by whom: Was “too little” or “too much” done in “response”? What did authorities know and when? Were plans abandoned or activated? Was it all premeditated? And if so, to what end?
In truth, there is little difference between two corresponding assertions:
Authorities didn’t know what they were dealing with and were caught off guard or underprepared for the virus (e.g., didn’t lock down soon or hard enough, early detection systems failed, the world was fooled by China).
Authorities should’ve known better; they panicked and abandoned pre-existing pandemic plans (e.g., measures taken were deadly, leaders need to be prosecuted for funding gain-of-function experiments).
Both views are “wins” for those invested financially or professionally in preparedness industries.
An Off-Limits view, by contrast, incapacitates the pandemic/bioterrorism complex altogether:
There was no need for a response of any kind and no spreading viral threat. Certain plans were activated without cause (or for undisclosed reasons), very likely for nefarious purposes, and involved democide. Pandemics, as sold, aren’t possible and preparing for them is a waste of time and resources.
Whatever one’s current perspective, it should be clear that government is still trying to control the narrative from all sides—and going to great lengths to keep unapproved perspectives from making their way into the public square.
This matters because anything less than a complete dismantling of the entire pandemic narrative essentially leaves the central scientific and socio-political paraphernalia fully intact. The trope du jour “we need to be better prepared for the next pandemic” is embraced by too many dissidents and—as we’ve already asserted—ultimately makes reruns far too easy to initiate and execute.
Added 24 July 2020:
See Neil & Engler, 2024; Neil, Engler, Hockett, 2025. | Holding this view (as we do) does not constitute an endorsement of GoF. We assert such experiments should be banned because they are wasteful and potentially dangerous to the lab operators or persons in the immediate vicinity, irrespective of their inability to create spreading, pandemic-potential viruses.
h/t @mapperdan for locating this paper, and for observing that “early treatment” was a phrase used during H1N1, with Ebola, and in January 2020 with respect to seasonal flu.
Also explained in Hockett, 2024.
Including by government, e.g., Federal COVID-19 Testing Report: Data Insights from Six Federal Health Care Programs. 14 January 2021. U.S. Department of Justice. | Rough, E. Coronavirus testing for COVID-19. 14 October 2020. Number CBP 8897.
Described in Neil, Engler, & Fenton, 2025.
More speculative propositions involve the sequence and associated disease having entirely different origins. See Hockett, 2025.
Chomsky, Noam. The Common Good. Edited by David Barsamian, Odonian Press, 1998.
See also Hockett & Engler, 2025.
 | A guest post by
|
 | A guest post by
|
Helpful framework, much appreciated. I agree with the categorisation, though obviously I’m deeply into the Off Limits category, since there’s no scientific evidence for the existence of viruses, all vaccines have always been a useless and deliberate deception of the public and pandemic based control & assault systems have been actively rehearsed for at least 25 years on an international basis. I expect it’ll be used again, alongside other not-happening fear provoking deceptions such as climate change crises.
There is a Japanese concept called “mu” for dealing with dichotomies. When faced with the choice of, “Do you want the right horn of the bull, or the left horn?” The answer is “mu.” Neither. Because your choice is to reject the dichotomy.