
"Place of Democide" Differences in UK vs. US
Hospital protection racket on both sides of the pond?


Commenting on this article via Substack Note,
said something important I want to capture and react to:This is a brief but solid summary of what happened to many people in countries which imposed absurd and obviously dangerous medical protocols on people in hospitals and care homes. This featured heavily in UK but not in Germany, for example, in 2020.
I have the impression that the hospital treatment route was particularly heavily employed in USA, while in UK, I have the sense that the care homes treatment route predominated.
This might be because the more heavily medicalised system in USA meant that they had a lot more mechanical ventilation beds per head of population than the UK had, where instead we have a large population of elderly people resident in privately managed care homes.
Is Dr Yeadon’s impression about the U.S. versus the U.K. correct - and does his hypothesis about the reason for the difference “work” with respect to spring 2020 (the timeframe I investigate)?
United States
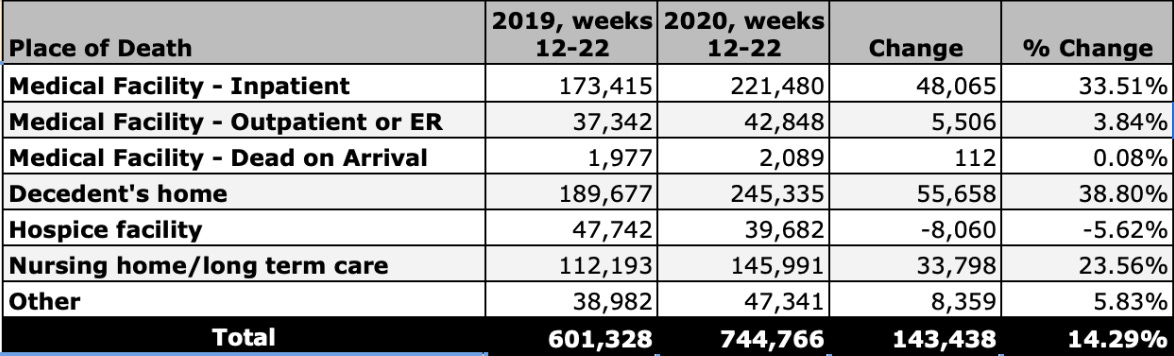
During the spring of 2020, U.S. hospitals experienced more excess deaths—and more COVID-attributed deaths—than nursing homes and long-term care facilities. Notably, deaths at home saw the greatest increase during the first wave.1 Based on my study of this period in New York and other cities, there is reason to believe that sudden changes to ambulance protocols, redirection of 911 calls, and “shell games” involving how deaths in hospices, nursing homes, and private residences were classified may have contributed to the patterns.2
Source: CDC WONDER
In ‘pinpoint pandemic’ locations like New York City/Metro, Chicago, and Detroit, many nursing home residents were sent to hospitals and never left. Unlike nursing homes, hospitals were financially incentivized with federal funds for diagnosing "COVID-positive" patients.
With some exceptions, when states were required to report nursing home COVID deaths, no distinction was made regarding where the deaths actually occurred.3 To my knowledge, no federal data source tracks nursing home or long-term care facility resident deaths based on their actual place of death.
These residents, along with existing hospital patients, may have been used to stage the sudden spread of a novel respiratory pathogen. (General steps outlined here.) It is truly perplexing that there has been virtually no push for investigations into what happened in U.S. hospitals and Emergency Medical Services during spring 2020—starting with New York.4
United Kingdom: England/London Focus
UK care home deaths during “the first wave" have received a fair amount of significant attention, partly due to guidelines that encouraged midazolam use [NG163] and discouraged antibiotics [NG165] for “managing COVID-19.5 There’s been less media coverage of the Scottish COVID-19 Inquiry, but it has delivered very damning evidence of euthanasia and maltreatment in care facilities.
Wave 1 place of death data for England show care homes as a place of death saw the highest percent-increase from the first week in the dataset to the peak, so a focus on what happened inside is clearly warranted.6
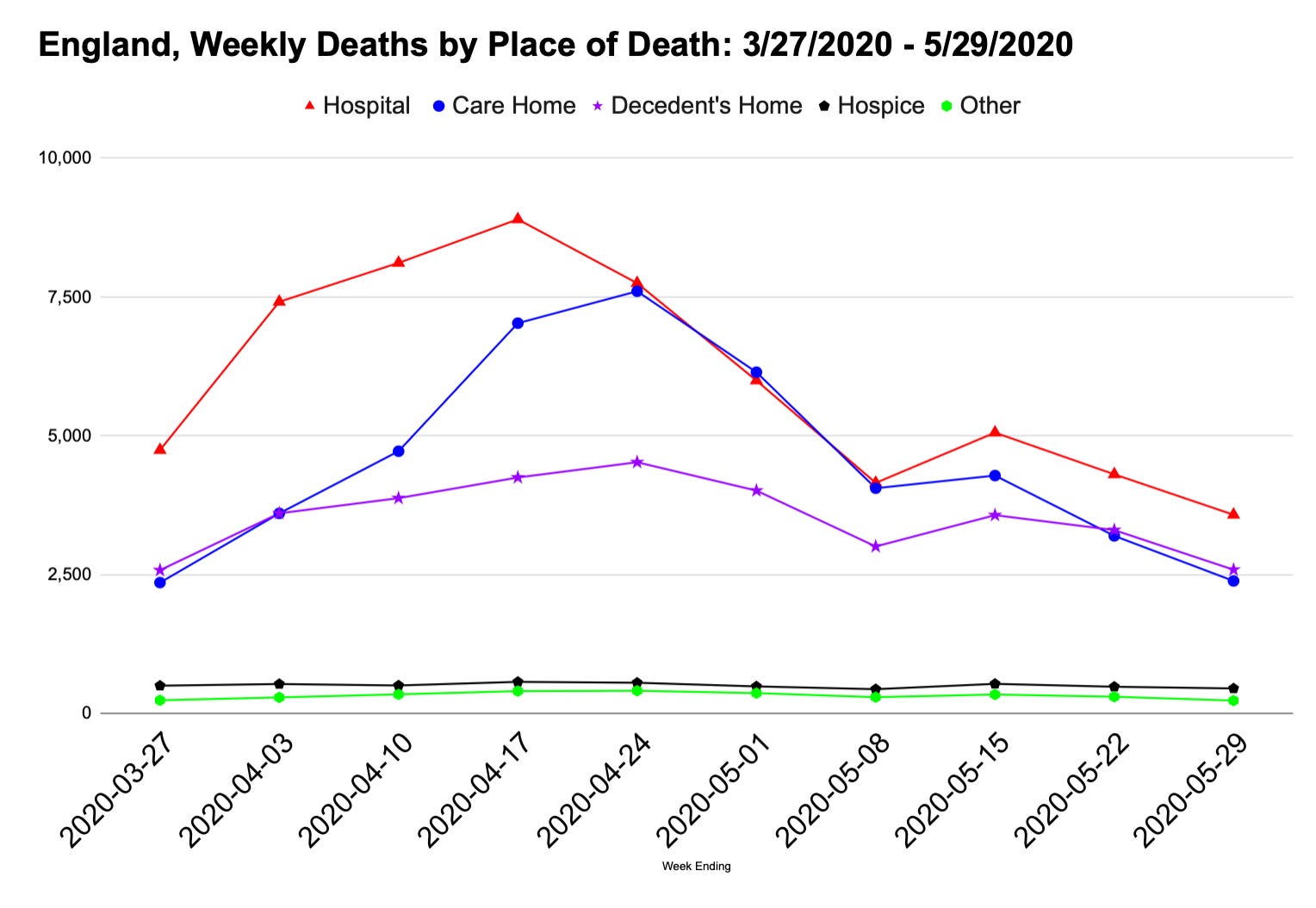
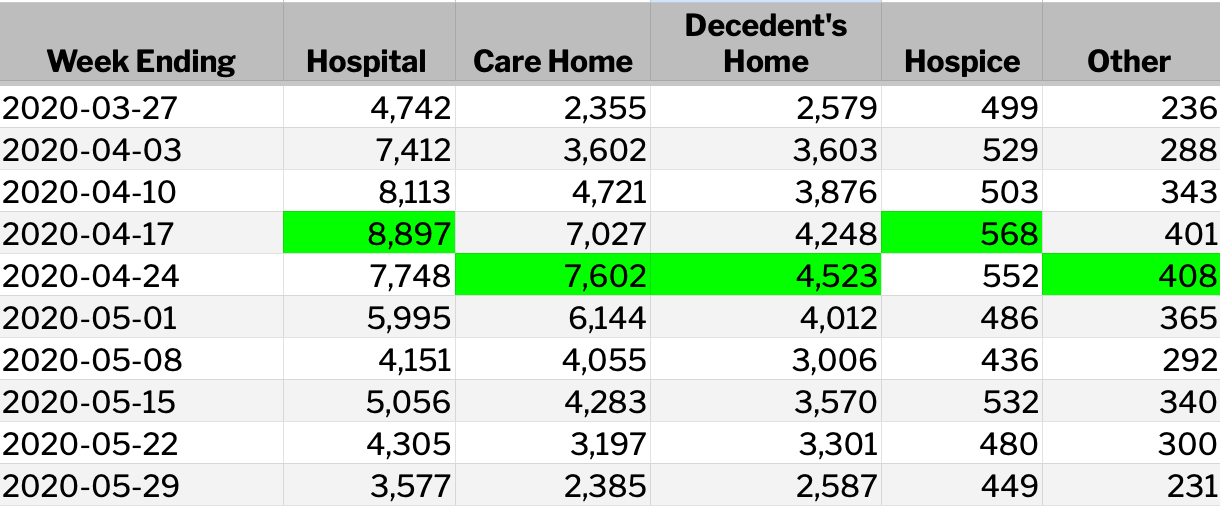
However, it was deaths in hospitals that rose first and most steeply after ‘lockdown’ orders were issued. Deaths in hospitals peaked a week before deaths in care homes and personal homes.
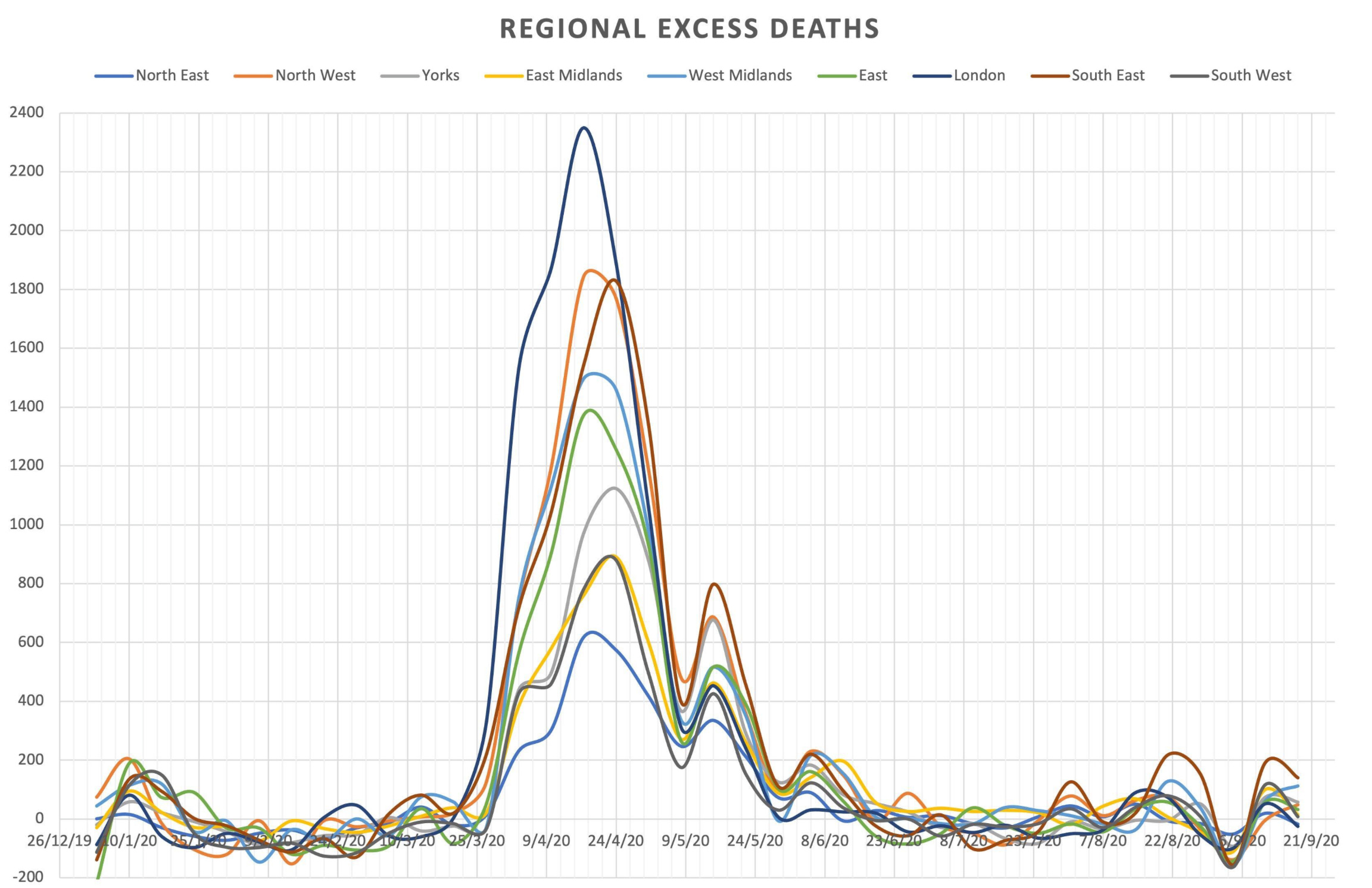
Examining regional excess death curves—and place-of-death data as shown in proprietary maps shown by Todd Kenyon here —suggests that the steep rise in hospital deaths may have been driven primarily by hospitals in London. The speed and magnitude of London’s curve is on my shortlist of suspiciously fast events.
Source: 1 July 2022 tweet via
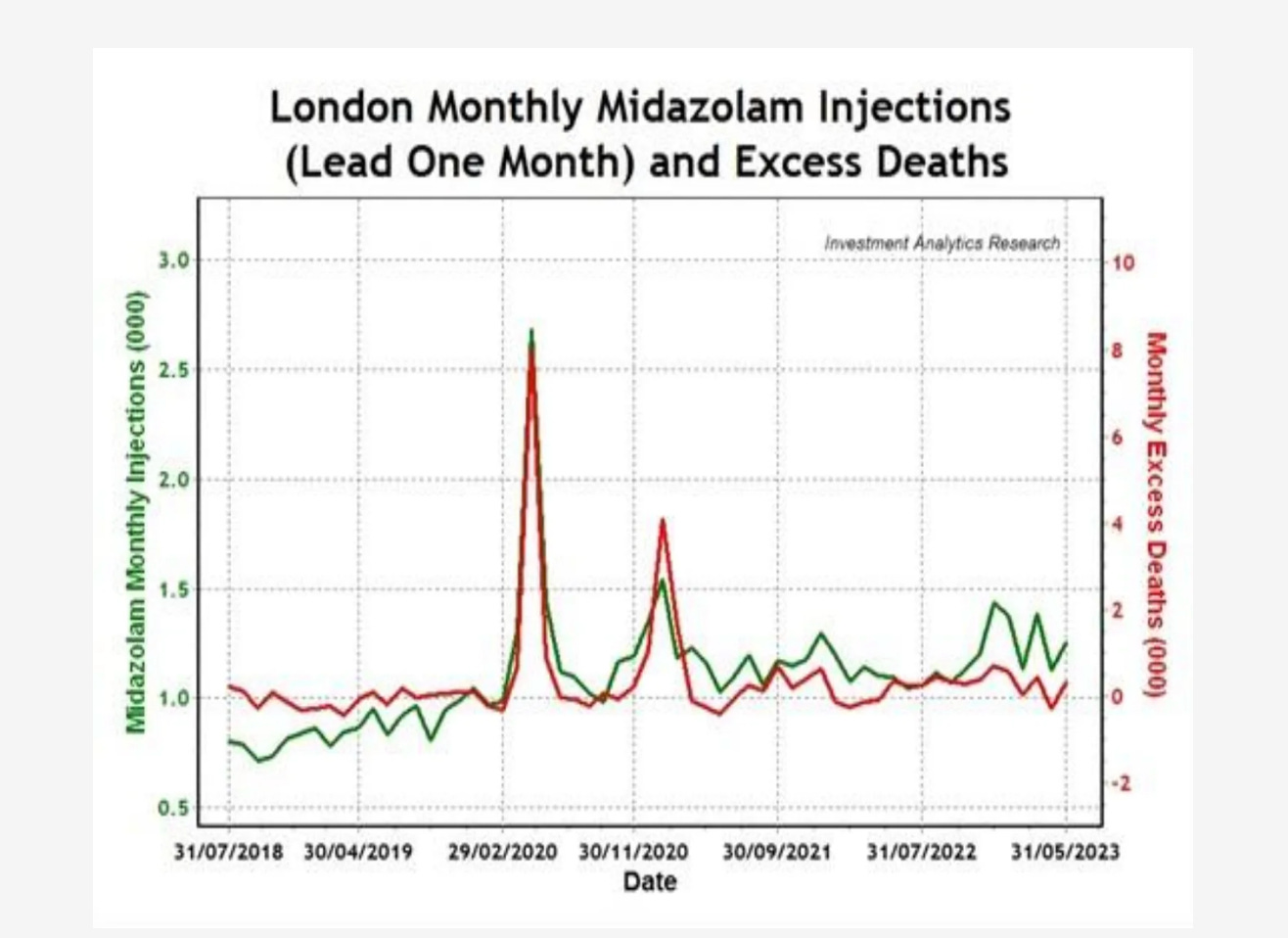
As early as July 2020, The Daily Mail was “disclosing” heavy use of midazolam in care homes, but said nothing about use of the drug in hospitals. Data reported by Wilson Sy (below) shows a strong correlation between monthly midazolam injections in London and excess deaths in 2020, though the figures are not broken down by setting (hospital or care home).
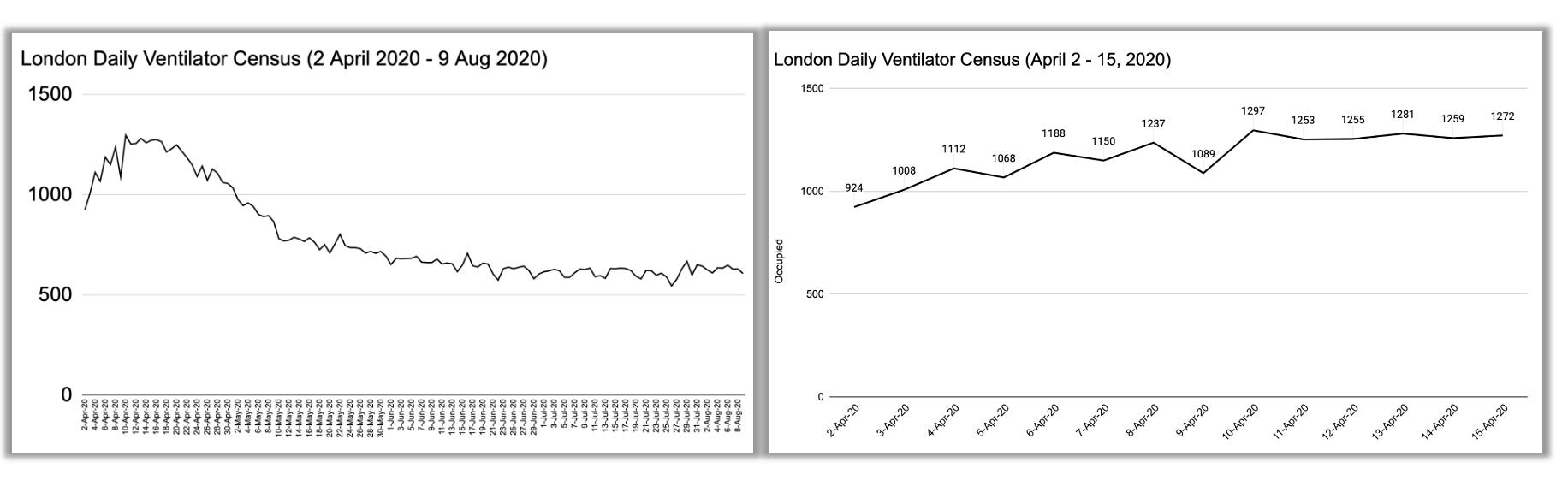
London’s daily ventilator census lacks a baseline, yet it still suggests that high doses of paralytic agents were used to intubate patients. Any genuine inquiry into the spike in London deaths should start with hospitals.7
Better Care Homes Than Hospitals?
All of this to say, I believe Dr. Yeadon’s impression that the US employed a “hospital treatment route” and the UK predominantly used a “care homes treatment route” is warranted, with two caveats:
In large cities like London (and New York, etc), deaths in hospitals rose first—likely due to the greater number and diversity of “damaged ships” in these urban “harbors” compared to care homes, and the expediency of the measures applied in hospital.
In the U.S., the hospital treatment route involved transferring nursing home residents into hospitals—often unnecessarily.
Regarding ventilators, increased use of the devices was never necessary anywhere, as no new pathogen was causing a novel illness spreading person to person. Where and when ventilators were used as “treatment” for “COVID” patients, they effectively served as a weapon in (simulated) “war” against an alleged invisible enemy.
Although mechanical ventilators can create complications that lead to death (discussed here), during 2020, government-directed use was effectively a “cover” for the delivery of drugs that euthanized patients who tested positive for the agent called SARS-CoV-2 - including patients already in hospitals before an emergency was declared.
While it’s important not to minimize the democidal policies enacted in care homes (or ignore the findings of the Scottish Inquiry), it’s difficult to overlook that focusing on nursing homes/care homes has had the effect of directing attention away from hospitals.
After all, isn’t it easier to say that care homes were “the real problem” for failing to control the “spread of the deadly virus,” while hospitals did everything they could—despite challenges like lack of resources or being “caught off guard”? People already have low expectations of care homes. By allowing them to bear the blame, the narrative supports the idea of a spreading virus while protecting hospitals. Losing faith in hospitals would be far more threatening to both the government and the immediate health of the general public than losing (more) faith in care homes.
In the U.S., the narrative for spring 2020 centers on the idea that COVID-positive patients discharged to hospitals “spread the virus” in nursing homes. A similar storyline exists in the UK, but there is also an impression that care homes killed residents by not sending them to hospitals in time, or when they should have.
In reality, fragile and government-dependent groups of people were “damned” either way during the initiation of Operation COVID. It wasn’t a novel pathogen that killed them—it was drugs, DNR orders, maltreatment, neglect, inappropriate or unnecessary transfers between facilities, and other factors. Perhaps it’s easier in the UK to administer midazolam in a care home setting than in an NHS hospital, whereas in the U.S., such injections are more commonly given in hospitals? I leave it to those familiar with the relevant policies and laws in each country to comment on any differences along those lines.
Differential Democide?
People on the edge of life - what I’ve called ‘precipice populations’ - were at risk of death via iatrogenic measures in spring 2020. Whether a hospital or a nursing/care home was the riskier place to be (mal)treated as a “COVID patient” was dependent not only on country, state, or city, but also on where someone ended up being suspected of or determined to be infected with the newly-named coronavirus.
What Mike Yeadon has sensed and hypothesized is crucial. While it may seem like a “distinction without a difference,” it could point toward advance-planned democide. Any directed operation would have to account for differences in restrictions, psychological priming, legal limitations, and other factors across the countries involved.
Headline edit 29 July 2025
ADDED 26 February 2025: Chicago-area example
"Informed Assent"? A DuPage County (IL) DNR in Spring 2020

A story from DuPage County, Illinois, early in the ‘pandemic emergency’ illustrates how government-directed messaging and protocols influenced doctors to make ethically questionable decisions.
Excess in these weeks was driven by certain metro areas. See figure 1 for hospital deaths in those areas versus the rest of the U.S.
In addition to (or even instead of) factors that are presumed but not as well-supported by different kinds of time series data or contemporaneous events as people think. Examples include extreme fear or “panic” and “despair”.
This was at the center of the Andrew Cuomo “nursing home scandal,” which has always been something of a distraction from what happened in New York City hospitals (explained here).
The House Select Subcommittee on the Coronavirus Pandemic nothing about a need to investigate hospitals, nor did a document that informed the committee’s work. If new HHS direct Robert Kennedy, Jr. has spoken to the issue, I’ve missed it.
See also this article.
The dataset I was given begins with the last week in March 2020. A more complete timeseries would be appreciated.
….and directives given to paramedics, in light of increase in calls for help concurrent to a significant OHCA event, shown here: https://www.woodhouse76.com/p/did-london-really-see-a-200-increase
I remain distressed that few to no noisy physicians have emphasised to the general public that sedation, intubation and mechanical ventilation are inappropriate treatments for patients who are conscious, breathing through an unobstructed airway (the opposite of such as a near fatal asthma attack) and have no injury to their chest (such as can occur in stab wounds, other causes of pneumothorax & crush injury).
If such patients had a low and falling blood oxygen saturation, the appropriate treatment would be an oxygen mask or nasal cannula so that they breathe from air enriched with oxygen to some extent.
The mechanical ventilation story was pushed very heavily where I was in UK, early in 2020, to the extent you could not have failed to be impressed by it. There was talk of a need to immediately close the gap between capacity and need, with something like 20,000 ventilators.
Recall the absurd situation where vacuum cleaner and vehicle manufacturers were being spoken of as potential sources for jury-rigged ventilators.
These machines, when used appropriately (eg surgery accompanied by deep anaesthesia, after head injury or poisoning, where the respiratory reflexes are blunted, severe burns and other conditions where injury is so severe than medically-induced coma is a humanitarian decision) is life-saving.
It’s a complicated piece of machinery and anyone with the first knowledge of them immediately realises that rapid production of ventilators is camel through the eye of a needle style impossibility. Not even close. Furthermore, it’s a discipline all of its own to know how best to “fly” the patient and recognise early if things are turning bad. So even if there really had been a need for all these machines (there definitely wasn’t), the lead time for producing those kinds of numbers would be, I suspect, in the years not months. And we’d still lack the skilled staff to use them.
I could write a long essay on how the knowing misapplication of mechanical ventilation to helpless patients in hospital is murder.
It’s long past the time when regular doctors, but at least pulmonologists, critical care specialists and consultants broadly in general medicine should be setting into the record views along these lines, providing they’re correct.
WHY are they not doing so? Those who know that wrongdoing was everywhere have an obligation to share what they know in order to reduce the risk that it’ll happen again.
I think it’s highly likely to happen again because the advantages to the perpetrators of doing so are strong, particularly in the context of respiratory illnesses.
It takes only a slight disruption in care, routine, and attention to throw fragile elderly folks (and some fragile younger folks) over the edge. The disruption in Spring 20 was far from slight. The US specializes during normal times in keeping these people barely alive, matrix-like, for extended periods so they can keep feeding the machine. So wherever these folks already were, many succumbed. The ones that actually made it alive to hospitals already had their death sentence signed upon admission. Its not hard to see why many would die immediately after the insane measures were implemented. I have seen no evidence that hospitals did anything beyond covering their asses. Workers had been propagandized to believe their own lives were in grave danger. Sick fragile folks were an easy sacrifice.