
Open Letter to Pierre Kory Regarding His Spring 2020 Experiences in Madison and New York City


In this open letter to Pierre Kory, also emailed to him directly, I address his
perception of COVID-19 as a new disease and cause of death requiring special treatments;
speedy elevation to national prominence and audience with a U.S. Senate committee in May 2020, despite limited experience treating COVID-19 patients;
claims about flu & COVID, flu patients in the ICU, and the 2019-2020 flu season;
impression of hospital activity and deaths in other U.S. cities compared to New York City in spring 2020;
lack of curiosity and interest in underlying causes of death among younger adults during the New York City mass casualty event;
language for describing his experiences in spring 2020 COVID-19 event;
reaction to the possibility that the federal government used New York City for a staged event, simulation, or “live” military exercise; and
resistance to calling for an investigation of what occurred in New York City hospitals before he arrived at the end of April 2020 and during his 4-5 week tenure.
August 8, 2024
Dear Dr. Kory,
Good day.
Our exchange began when two associates and I engaged your claims about COVID-19 being a new and unique disease. In response to your rebuttal, we concluded that nothing in your academic publications, articles, stories, testimonies, and other written comments challenged our hypothesis that a novel deadly respiratory virus spreading from person to person is not responsible for what you or other doctors observed in the spring of 2020. You declined to respond again in writing.
Separately, I posed questions about your experiences in the first five months of 2020, with a focus on what you saw at UW-Madison and in New York City. You graciously recorded responses to my questions, sent those videos to me, and granted permission to share publicly, which I did, with transcription.
To anchor this dilatory and lengthy letter, I created a timeline for the period of interest based on your videos, things you have said/written elsewhere, and other events & sources.1
You spent six weeks in February & March 2020 preparing the UW-Madison hospital for COVID-19.
You were promoted by the medical school you attended on 3 March 2020.
The WHO declared a pandemic on 11 March 2020, the U.S. declared a national emergency (and activated the Stafford Act) on 13 March 2020, and the President announced “15 Days to Slow the Spread” on 16 March 2020.
You co-founded the organization that became Frontline COVID-19 Critical Care Alliance (FLCCC) in March 2020 (date unspecified).
In late March 2020, you were “on a sort of half leave” and had “ceded a position to a colleague” due to needing to handle a family member’s health issue.2
You were constantly on individual or conference calls with doctors in NYC and other cities in March and April 2020.
Your first COVID patients in Madison arrived in early April 2020. You were “not on service taking care of COVID patients” but were “in the unit, with my colleagues, doing ultrasounds” because you are an “ultrasound expert” and were “finding clots.” You also said your colleagues were presenting COVID cases to you and you “knew” the cases but were not personally in charge.
When the FLCCC group was formed, you spent time contributing to media. For example, on 7 April 2020, you and other FLCCC doctors released the video “Early Intervention Protocol for COVID-19 Can Save Lives”. An 15 April 2020 FLCCC press release quoted you.
You didn’t say how many total COVID patients you encountered or treated in Madison but mentioned there were at least eight (8) patients in the UW-Madison COVID ICU in April 2020 and that you “think” you “started to use the main ICU” for COVID patients. There was never a surge, you said, i.e., the “onslaught” of COVID patients you were told to anticipate never came.
You requested and were approved for a month-long Continuous Leave without Pay from UW-Madison for “Exceptional Personal Reason.” On the form you said the reason was “humanitarian leave to support NYC critical care heads.”3 The start and end dates listed are 24 April 2020 and 27 May 2020, respectively.
You said you arrived in New York on 26 April 2020 and started at Mount Sinai Beth Israel on 27 April 2020, which is same day your request for humanitarian leave was approved. Official data show deaths in NYC hospitals had peaked more than two weeks before you arrived.
You recalled 16 patients in the Beth Israel ICU that you “took over” at the end of April 2020 - many of whom “had been admitted days to weeks before” and most of whom died. Elsewhere, referring to Beth Israel, you said you had an ICU with “24 patients with the same chest x-ray.”
Sometime between 26 April - 2 May 2020, you were contacted by Chief of Staff for Senator Ron Johnson (R-WI) about testifying at at U.S. Senate Committee on Homeland Security & Governmental Affairs “Roundtable” on COVID-19. You said the interest in you versus in an NYC hospital employee was due to your affiliation with FLCCC and you being the chief of critical care services at UW-Madison.4
You testified to the Senate committee on 6 May 2020, the same day you tendered your resignation from UW-Madison. Among the statements you made: “The mortality and morbidity rates of this disease are unprecedented. I’ve been doing critical care for a decade and a half. I do not see mortality rates associated with any severe illness that I see in this one.”
You said you had a “handful” of new admissions at Beth Israel in May, most of whom were “the chronic severe COVIDs on vents.” By the end of May/early June 2020, COVID patients at Beth Israel had disappeared.
You returned to Madison in early June 2020.
My reactions follow:
1. Nothing in your video responses persuades me that the patients you saw in spring of 2020 were sick with something new or heretofore unseen in the clinical setting that necessitated special treatments.
Hypoxia is ill-defined & subject to measurement error, clotting has numerous potential causes, and kidney failure is quite common among the elderly infirm and other sub-groups. The sudden appearance of patients having “similar CAT scans” means very little and, if anything, is more suggestive of orchestration or of characteristics common among care home residents or people already in the hospital who are close to death than of a disease that wasn’t presenting itself until it was given a name and doctors were told to test for “it” and ascribe whatever symptoms of conditions the patient had to “it”.
You said your hospital in Madison tested every patient who came to the ED or was admitted as an inpatient for COVID-19 but rejected the idea that COVID was merely a positive result on a PCR test [for SARS-CoV-2]. At the same time, your description of things you were seeing challenges your claim that COVID is a unique disease necessarily caused by a newly-discovered coronavirus:
“I could care less about the positive test. I took care of patients with negative tests who had COVID. You guys think that I’m like, you know, only a positive test determines COVID. These patients were reproducibly appearing in patterns and certain, um, distributions of abnormalities on the X-rays. I mean, it was really very reproducible the way they were presenting. They were getting severely ill… You wanna call it COVID or not, I don’t care what you call it. I don’t care about the PCR test. The disease was severe, reproducible, and they were massive numbers of patients and they were filling and depleting ICU resources. I don’t care what pathogen it was and what test it was. But the disease was absolutely reproducible.”
The “patterns” and “distributions” you described are rather vague and could apply to many conditions. Should I interpret your belief that COVID is a disease independent of a positive test to mean that you think there may be other viral agents or factors that can induce “the disease”? Similarly, I don’t understand how you can characterize long COVID as a “new name” for an “old disease” - myalgic encephalitis chronic fatigue syndrome (MECFS)5 - and say the incidence of long COVID is evidence of novelty.
I sense you are trying to convey that good doctors treat the patient, not the test result. However, it’s hard to ignore that you began to “see” patients with like-conditions after your hospital had been “readied” for COVID patients and started testing everyone for SARS-CoV-2. Patterns in your and colleagues’ clinical observations did not precede the advent of mass testing and other protocols.
It doesn’t sound like you had primary responsibility for treating COVID patients in Madison in any case, due to other duties you held. You said,
“So did I ‘attend to COVID patients as well’? Not as the prime–when you’re asking about the early weeks, so a lot of those briefings were before our first COVID patient. We were just - it was new policies, protocols, what to do when they arrived. I was working with a therapeutist committee, coming up with a treatment protocol. I got IV Vitamin C on the protocol. But I was not on service taking care of COVID patients, but I was in the unit, with my colleagues, doing ultrasounds. I’m an ultrasound expert, so I was examining them. We were finding clots. I was doing lung ultrasounds. So I was heavily involved. My colleagues were presenting the cases to me and so, like, I knew the case. But I was not personally in charge.”
The treatments you were condoning via FLCCC in spring 2020 appear to be treatments that you and others had already been using and studying for other conditions and patient types.6 I am not a medical doctor and haven’t taken much interest in the COVID-19 treatment conversations. Reviewing your testimonies, contemporaneous documents, and studies submitted for publication before March 2020, however, it seems the therapies you and your colleagues advocated in those early months were essentially what was being used in “critical care” with patients suffering from ARDS, sepsis, and other conditions common in certain populations (e.g., the MATH+ protocol).7
I asked if the treatments you were advocating and using in those weeks were successful and you said no, using the example of IV Vitamin C:
“I know hospitals were using IV Vitamin C. Some of the - some of the ICU docs who were on service used it because it was on our protocol [at UW-Madison]. Didn’t last on our protocol very long, by the way. That’s one of the reasons why I left University of Wisconsin is because the Dean got the Chair of Medicine to remove IV Vitamin C. So I wouldn’t say I was using them successfully. And then I would add to that, my colleagues Northwell Hospital System on Long Island, which is right outside New York City, they had a systemwide protocol using very high doses of IV Vitamin C. It really didn’t do much in that first wave. I know the data now shows that it helped reduce pretty much every important adverse outcome. But back then they weren’t seeing huge impacts from a high-dose IV Vitamin C.
I’m unclear as to what changed between "the first wave” and later waves that resulted in “huge impacts” from a treatment that “didn’t do much” initially.
Your claim in one of the video responses that “no treatment was being given” in NYC hospitals is difficult to believe, unless this is a critical care euphemism for hospice patients or others at the end of life who were PCR-tested due to protocols or for research purposes and would not have been “treated” regardless. In the event you witnessed non-treatment constituting a breach of ethical codes, I trust you filed the appropriate complaints.8
2. The number of COVID patients you had personally treated from entry to discharge was very limited for someone who was quickly elevated to national prominence as expert on treating “COVID.”
To be perfectly frank, I’m at a loss as to why you were selected to testify in early May 2020 about the efficacy of treatments for a “new” disease when your experience treating it was so limited. Your statement to the Senate Committee about COVID-19 being one of the worst diseases you had seen in terms of morbidity and mortality is hard to reconcile with how few patients you had seen or treated successfully by that point.
Your trajectory from doctor at UW-Madison to doctor testifying before a Senate committee was incredibly fast. You said your decision to go the New York was multi-factorial.” You weren’t seeing a lot of cases or a “surge” in Madison but were hearing from colleagues in New York about everything that was happening there and reading email solicitations from organizations like the Society of Critical Care Medicine.9
Your request for “humanitarian” leave from UW-Madison (shown below) corroborates your general motivations. I note that no specific hospital is named - only the task of “support[ing] NYC critical care heads.” If your memory is correct and you arrived on 26 or 27 April, it appears your request was post-dated and approved after your arrival (i.e., submitted on 27 April and approved 28 April).
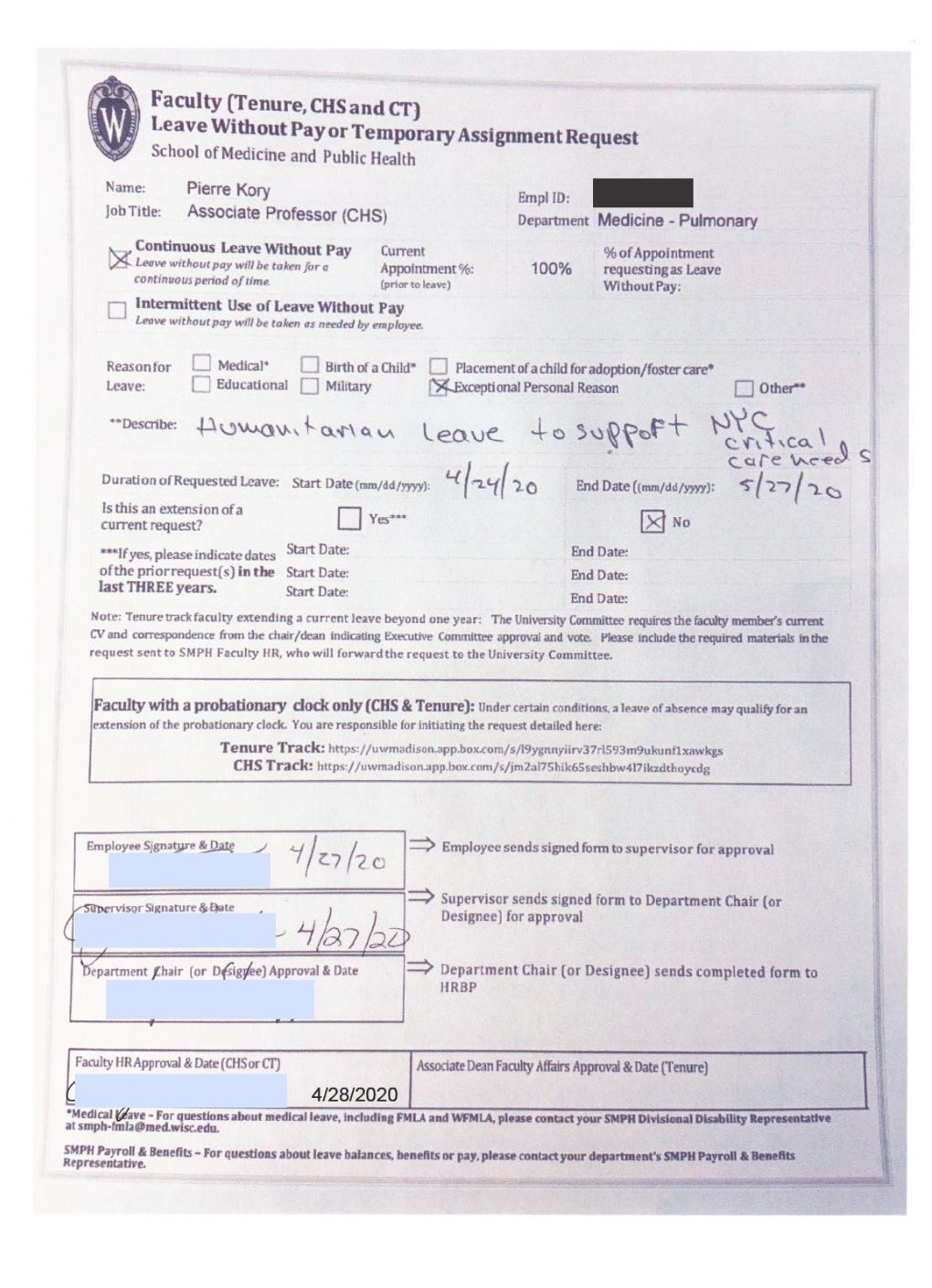
Obtained via FOIA request from UW-Madison. Signature redactions are mine, not UW’s.
Unlike you, I find it very strange that Senator Johnson didn’t call an administrator or doctor who was an employee of a public or private NYC hospital or system to testify at the roundtable event. By his own admission, Senator Johnson did want to know what happened in New York, in addition to knowing about treatment. Wouldn’t it have made more sense to call the head of critical care at Elmhurst Hospital, or an administrator from NYC Health + Hospitals Corporation? On the day you testified, media were reporting more than 31,000 “coronavirus” deaths in the tri-state area alone. It made no sense to summon you unless the Senator or someone else sent you to New York, which you said was not the case.
Your activities prior to May 6, 2020 did not involve having primary responsibility for COVID patients from admission to discharge, as might be expected of an expert witness. It was apparently your engagement with the promotion of treatments more than treatment itself that placed you in front committee as a spokesperson for treating a newly-announced cause of death. This included remdesivir, which you told me is a “joke of a drug” in the hospital but beneficial as an outpatient prescription - a sentiment consistent with your May 6 testimony. What all influenced your early recommendations about remdesivir, I am not sure, but I note John Ioannidis also submitted testimony which spoke of the drug promisingly.10
You said the patients in the ICU you “inherited” in New York “had been on vents for a couple of weeks and they were pretty much non-rescuable.” The conditions you describe sound like a research study or experiment more than they do medical care, as though you walked into conditions set-up as a living morgue:
“I mean they were really chronically, critically ill and dying. So I basically oversaw a fair amount of death. I mean I threw the kitchen sink at ‘em and it didn’t really work that late in the disease. I was involved with the first attempt at a lung transplant. I had one guy who wasn’t intubated, he was on biPaP for about three and a half weeks, which I had never seen in my life before. I’d never seen someone on 100% full settings of biPaP for three and a half weeks. Never ever ever have seen that. And so I tried to get him a transplant and he – I did transfer him to a transplant center but unfortunately he died on arrival because of, um, machine malfunction on the way.”
Is it possible you were, without your knowledge, encouraged to go to New York in order to verify that something had occurred so that you could be tapped to testify on May 6? If not, I hope you can at least see how the speed and sequence of events invites speculation you may have been intentionally, if unwittingly, used by the U.S. Department of Homeland Security or another agency.
3. Your insistence that COVID is not anything like flu is at-odds with your lack of experience with treating flu in the ICU and lack of awareness about variables reported in flu surveillance reports, widespread characterization of COVID as a pneumonia in early 2020, and reported severity of the 2019-2020 Wisconsin flu season.
You repeatedly insisted COVID is not flu and cited your ICU experience as circumstantial evidence that COVID is much more severe than flu:
“I never see flu in the ICU. I mean, my entire career I’ve seen flu like four or five times. And I think three of the four were pregnant. I don’t know what a severe flu season – that’s for epidemiologists and people out in the community. But in the ICU, there’s no such thing as a flu season. I just don’t see a lot of flu in the ICU.”
Um, I really–but the “no new novel pathogen” is so bonkers and out there. That’s the only thing that I think you guys have to admit you’re wrong and come up with a new theory to explain what you can’t figure out with the data, ok? But ‘no new novel pathogen’ is just bonkers. Bonkers. I mean, I’m literally an expert in acute respiratory failure. I’ve never seen a pathogen like that. Flu and vaping? It’s just a joke. I can’t tell the difference between flu and a novel pathogen? Like I told you, flu doesn’t come into my ICU. Ever. Ever! When I ever, like, I told you - in my career, four or five cases of the flu and you guys are like, “this is an influenza-like illness.” Yeah, this is nothing like influenza.
If you didn’t often see patients who were sick with or had tested for flu, does this mean your belief that COVID is nothing like flu is a matter of presumption versus observation? Did you assume COVID can’t be flu because you don’t usually see flu patients in your ICU? If you don’t usually see flu patients, how confident can you be about the distinction between (for example) chronically ill elderly patients who test positive for influenza versus chronically ill elderly patients who test positive for SARS-CoV-2? Is there really a difference? If so, can the differences be attributed to other factors?
The tone of your responses suggested the idea of flu in the ICU is patently absurd to entertain, but my question is rooted in fact, not in wild speculation. Flu-associated ICU hospitalizations are a reported variable in national and state weekly surveillance reports (Wisconsin included). Chicago’s flu reports show the number of people in the ICU with flu on ventilators. You may recall the Chinese initially called the coronavirus they said they discovered “Wuhan Seafood Market Pneumonia” virus and the disease “Novel Coronavirus Pneumonia (NCP),” which indicates they associated a genomic sequence with a “flu-like illness.”
You almost certainly encountered patients with pneumonia in the ICU on a regular basis, even if other conditions or ailments brought them there, correct? Per the CDC’s EPIC study in 2015, a high proportion of pneumonia hospitalizations don’t identify a “causal” pathogenic agent or single agent. To the extent that influenza viruses cause pneumonia, it is quite possible you did see much more flu-associated pneumonia in the ICU prior to March 2020.
In fact, a story on the 2019-2020 Wisconsin flu season contradicts some of your perceptions:
Although its final months were overshadowed by COVID-19, the 2019-20 influenza season was serious across the United States and within Wisconsin.
Thomas Haupt, influenza surveillance coordinator at the Wisconsin Department of Health Services, said the season was among the worst since the agency began keeping records, and came with some unexpected twists.
"It was a bizarre season," Haupt said. "It started off with the influenza B virus being the predominant virus until the first part of the year. Historically, when you have influenza B viruses, they usually come after influenza A."
There were around 4,400 hospitalizations for influenza across Wisconsin between Oct. 2019 and April 2020, with the most acute numbers reported after influenza B strains began to circulate in mid-December, and worsening as infections of H1N1 and other influenza A subtypes started to increase in early January. Two of the four different types of influenza viruses cause significant illness in humans — type B is generally responsible for seasonal influenza, while type A is often associated with more virulent and pandemic-level outbreaks.
You may not have seen flu in your ICU at UW-Madison, but other ICUs in the state clearly did:
"Our rates of intensive care admissions and ventilation were very close to being at the highest that we've ever had," Haupt said. "With the exception of the 2017-2018 season, and that was the season that the [Centers for Disease Control and Prevention] is calling one of the worst and most severe we've had in the last 40 years."
4. You’re not grasping how much of an outlier New York City’s spring 2020 death event is — to the point it affects your credibility.
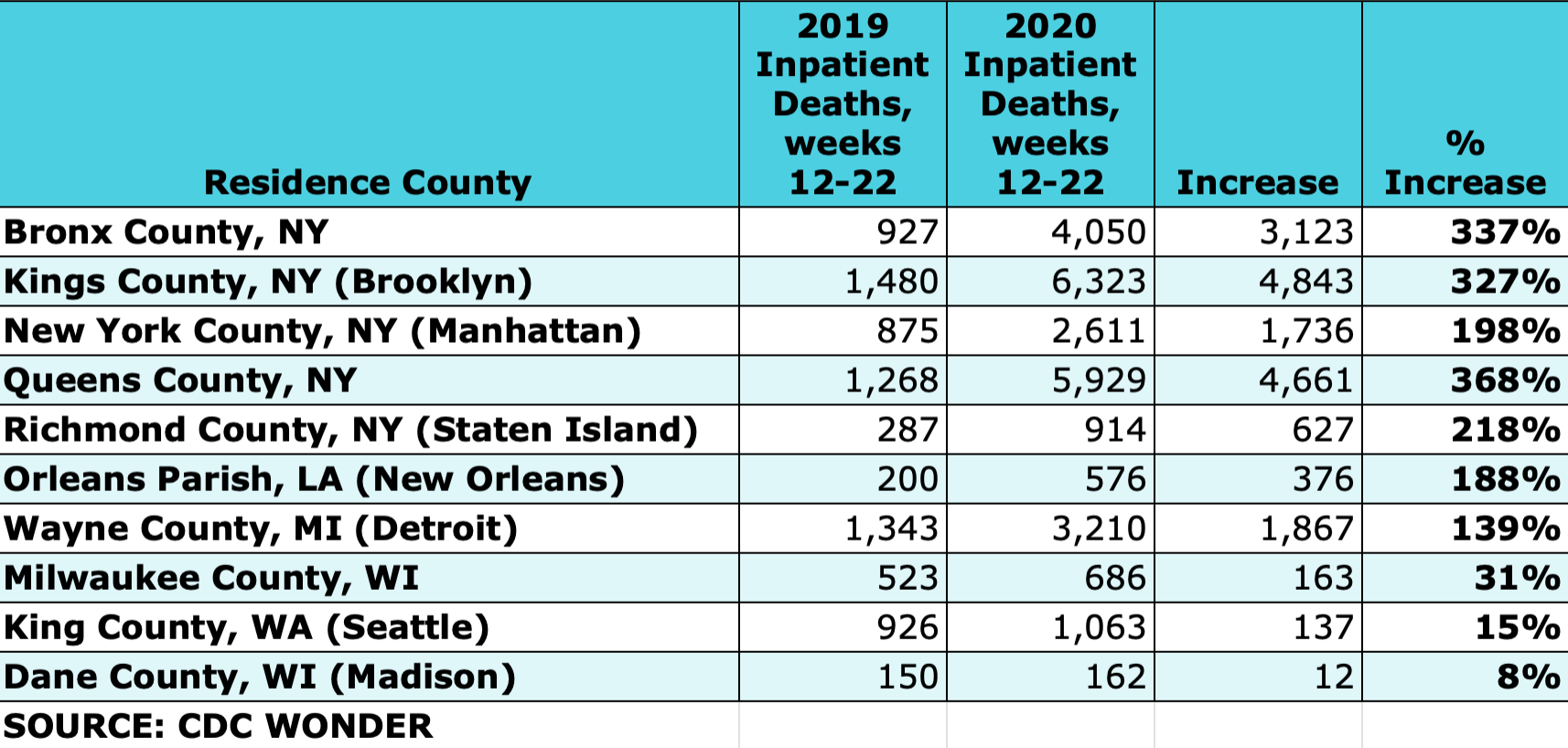
You mentioned Milwaukee, Seattle, Detroit, and New Orleans as cities that “got absolutely hammered” or “got hit hard too” with “a lot of sick people entering hospitals with this disease” as told in “huge WhatsApp groups with doctors all over the country.”11
The table below shows weekly inpatient deaths during the weeks of spring 2020 event for the places you mentioned, plus Madison, compared to the same weeks in 2019. New Orleans and Detroit each experienced well over 100% increase, but all five boroughs of New York reported over 200%, with Queens approaching 400%. It’s an outlier by any definition. This is basic descriptive data and doesn’t require high-level math skills to comprehend. You saying, “You guys keep thinking that New York is so unique” suggests that you either don’t want to look at the numbers or haven’t taken the time to process it and reflect on the implications.
New York City hospitals claim to have lost the near-equivalent of every normally-available inpatient bed — almost 20,000 inpatients — during a time when peak census was just over 20,000 beds. I don’t think such an event has ever occurred in a U.S. city hospital system. (Indeed, I’m not sure it happened in New York and have said so.)
The things you were hearing on your calls were also “outliers”. You said, “I was on the phone every day with ICU directors in New York who were telling me how hammered they were getting. They were running out of ICU beds in rooms.”
In retrospect, does it strike you as odd that those directors were on the phone as their hospitals were under siege? How should we reconcile that with data which show the so-called “epicenter of the epicenter” hospital (Elmhurst) was not experiencing unprecedented patient volumes? Why then have we not heard from hospital employees four years later about what must have been a very traumatizing event in terms of death and body management? Why do so many of (what I call) the approved voices of the timeframe such as yours sound as if they followed a script?
Domestically, we weren’t hearing reports like those out of New York anyplace else. Your oft-repeated story about your “fellow” in Detroit is high on drama but low on plausibility. This isn’t to say the doctor didn’t tell you he was managing 50 patients on ventilators. I waited tables earlier in my life - as did you, per your book - so I understand that “frontline” workers in service industries can be prone to hyperbole when they are feeling stressed (e.g., “I’ve got like 20 tables I’m trying to manage right now!”). Did you/do you find it strange that he was being asked to manage 50 people on ventilators, especially as a fellow? (I do!) Is he able to provide first-hand testimony? Shouldn’t he be interviewed for a documentary?
The trouble with anecdotes in this timeframe is that third-party witnesses weren’t allowed inside hospitals. Patients were locked in and their loved ones locked out (relegated to iPads, like you said).12 A lot of what you reported hearing from doctors in other cities is simply hearsay, curiously similar to propaganda reported in news media, and uncorroborated by patients who survived. (“I Survived Being a Patient in a New York City Hospital in Spring 2020” would make a good t-shirt for a Times Square vendor - yet how many potential customers are there, truly?)
As for the Seattle area, not only is the inpatient death data at-odds with your perception, the sworn affidavit of Dr. James Miller about his experience at Providence Regional Medical Center Everett in early 2020 contradicts the reports you were hearing.
Globally, New York City’s death event was exceeded in magnitude only by provinces in northern Italy. The cities of Madrid, London, and Manaus (Brazil) also experienced incredible events that have yet to be fully explained or substantiated with decedent names and death records. The similarities & differences between Bergamo, New York, and Chicago are also puzzling.
5. You don’t seem especially concerned about the high number of COVID deaths among younger working-age adults in New York City and don’t believe it warrants an independent investigation of what occurred in hospitals.
One of the most puzzling and distinctive features of New York City’s event is the death increase and number of COVID-blamed deaths among adults under age 70. Most of those deaths occurred in hospitals.13 Although you suggested you saw some nursing home patients at Beth Israel, you reiterated that most patients you saw were not elderly:
“I had patients…many non nursing home patients. I just remember a lot of fathers, 48 to 52 on vents.”
“[You repeating my question] ‘Is it possible that the patients you saw were chronically ill patients that were transferred from nursing homes?’ No! I took care of taxi drivers and truck drivers. I remember I even had a patient that got transferred to us from the tent in Central Park. They had set-up, they needed more capacity and there were patients on vents in this tent in Central Park.14 One person got referred to me there. But they were not chronically ill patients. I mean, come on. I’m a doctor. I do this all day long. There was all sorts of patients coming in. There was no common theme. If–in fact, most of my memory is not of the elderly. Maybe the elderly died before they could get to the hospital. Most of them – I just remember 40s, 50s, 60s—even a couple of 30, people in their 30s.“15
The idea that “the coronavirus” presented a risk to younger people was prominent in the Federal government’s messaging and among elevated NYC healthcare worker voices during the spring 2020 event. Surely at this point you recognize that COVID killing younger adults en masse is inconsistent with both what was “known” at the time and what is acknowledged now.
Yet when you responded to my question about whether you think a formal inquiry of New York hospitals is warranted, if only on the basis of those younger deaths, you said:
“No. The hospitals, they just weren’t being aggressive. They were doing supportive care only and that was the terrible thing that they did.”
I find that deeply unsettling. If hospitals do a “terrible thing,” whatever the reasons or circumstances, shouldn’t it be investigated? Why would someone in your position not want to find out about why you saw men roughly your age dying of something that was said to be a risk to the elderly and chronically ill?
You showed similar disinterest in the vaping (EVALI) case "outbreaks,” which also skewed young and were first reported in Wisconsin. Despite the obvious similarities in symptoms, and acknowledging it made young people “quite sick” (including patients your ex-wife treated), you found it impossible to consider the overlap or potential connection between vaping illness & COVID or vaping illness, flu, & COVID. Respectfully, I don’t think it takes a medical degree to read this first alert in July 2019 from the Wisconsin DHS and see some hauntingly familiar symptoms. (You may remember this September 5, 2019 alert issued in Dane County.)

It’s possible there is no connection between EVALI and COVID, nor anything suspicious about the CDC’s last update to this page being just before the pandemic was declared, but your resistance to considering if they could be related is odd, given that your state of residencce was at the center of the original reports in 2019 - and (with Illinois) a focus of a subsequent NEJM study.
My colleagues and I never claimed vaping was responsible for thousands of deaths or that you observed vaping illness in the ICU and confused it with COVID. Yet in your response to us you contended COVID patients weren’t vapers and there wasn’t a sudden increase in sales of vapes in spring 2020. To my knowledge, systematic collection of COVID patients’ vaping habits did not occur. New York City’s massive home death toll, drop in home-death autopsies, and strange reports of blood clots and strokes in younger adults during the timeframe certainly leave room for under-investigated factors.
As for sales, figures in this CDC report show a significant increase in certain flavors and types of e-cigarettes in the last months of 2019 into early 2020.16 The ICD-10 codes for COVID-19 and vaping-related disorder are both emergency use codes and took effect the same day: April 1, 2020. Given the overlapping chronologies and lingering questions about the origins and causes of both, I see no grounds to dismiss or scoff at questions about or speculation regarding a connection — especially where the unexpected deaths of young people are concerned.
The same could be said for the massive rise in opioid deaths, which I did not ask you about but I fear has been minimized and, in some cases, conflated with/as deaths resulting from the COVID shot.
6. The way you speak about COVID in spring 2020 makes it sound more like a force of nature or a war than a spreading disease.
The preparations that you described your Madison hospital undertaking are consistent with what hospitals in many places reported doing or having done.
You said you and colleagues spent weeks getting ready:
“I was…preparing the hospital for an onslaught of COVID patients. Starting in, like, February. You know, when we started hearing reports of like New York and Seattle17 I spent probably six weeks with administrative and clinical leadership developing processes and things about PPE and running IV tubing through the walls and externalizing ventilator controls [so] that we didn’t have to go in and out of the rooms.”
“We were just using what we thought was the most efficient way to care for patients with a highly transmissible disease. We were making negative pressure rooms. We were cohorting. We made a COVID unit, which we repurposed. We tried to add beds.”
You said there was no guidance for how to “prepare” the hospital and that your hospital in Madison was “just using what we thought was the most efficient way to care for patients with a highly transmissible disease” when, in fact, there was quite a bit of contemporaneous guidance, not only from Chinese and Italian sources but domestically as well.
The nature of these preparations does not make sense. We are supposed to believe that preparing for the “arrival” of a respiratory virus is like preparing for a chemical or bomb attack or a natural force phenomenon that can be reasonably described in terms of “getting hit,” such as a hurricane, earthquake, or tidal wave? The idea that a virus “striking” a city is a timed event - like something that can be predicted and seen on Doppler radar - offends common sense.18
Some of you what said to me is evocative of a soldier hearing about enemy forces with heavy artillery descending hither & yon, with expectation of arrival in his own zone in due course. For example:
“We knew it was going to get to us at some point. New York, Seattle, Detroit, New Orleans. Like I was telling you, there were a number of cities and places that were getting hit.”
Attempts to describe the movements of a “spreading” virus are illogical given the geographic distribution of cases and deaths. I’ve found no place in the U.S. where hospitals were suddenly overrun with sick people, and there are many reasons to believe a good portion of “positives” lighting up dashboards (including in NYC metro) were people already in hospitals and care homes being tested and re-tested. New York hospital staff were tested in March and multiple times thereafter, according to current & former employees I’ve spoken to.
From the perspective of someone who accepts that person-to-person transmission of a fast-spreading pathogen was occurring, what is your explanation for why Madison, which isn’t far from the international travel hub of Chicago, didn’t see a case until April when Chicago’s first case was announced the third week of January?19 Or why Detroit, Denver, Cleveland, New Orleans, Minneapolis, Orlando, and Atlanta each fared so differently in those weeks?
In your written rebuttal, you guessed that “something nefarious contributed to the anomalous spread, something as preposterous as deliberate widespread release in certain targeted cities and areas.” Via video, you cited Robert F. Kennedy’s Wuhan Cover-Up book to support the idea that a point-release or attack on certain cities is possible and said, “This to me was a bioweapon and this is what happened…I just think that’s the only…it’s a reasonable hypothesis…”
A problem with declaring “Bioweapon!” is that it explains nothing in terms of timing or potential mechanisms. Pathogens escape from labs fairly often but don’t do much of anything, get far, or get far fast. Short of chemicals, gases, injections, and contamination events, achieving mass death simultaneously in specific places around the world is hugely difficult. Successful “bioweaponry” development involving coronavirus is (fortunately) the stuff of Hollywood fantasies, however unethical. Invoking a phrase
and used in their recent paper, there may be function claimed, but in truth, no function is gained.Moreover, you don’t need to go all the way to Wuhan to find a virus lab engaged in gain-of-function research. The virus lab at UW-Madison has been subject of debate and ongoing scrutiny over its flu virus gain-of-function activities.
As for whether a “bioweapon release” changes your view on the WHO pandemic declaration, you weren’t sure:
“Yes, I mean, I don’t know what to make of this. I don’t know why it happened. I don’t know why it transmitted that way, why it spiked in certain places. Um, but ahhh...it was becoming a problem in numerous areas of the world and and..in my…yeah…I think it was reasonable to call it an emergency, cause it was an emergency. I mean, we were getting overwhelmed.”20
Yet when I asked if you’d considered that what you saw in New York has alternate explanations that don’t involve a spreading coronavirus, you said,
“No. Period. End of story. No. This was clearly an infectious illness that was transmitted from person to person. Uh, and that’s it. That’s all I’m gonna say. This does not change anything. Why it spiked, why it came in waves, why there were so many different variants, why there was different morbidities, mortalities. I don’t have great answers to that.”
So, like me and many Americans, you struggle to apply what we are told by virologists, epidemiologists, public health elites, pandemic planners, and bioterrorism experts to what official data say and what occurred “on the ground.”
7. Your reactions to questions related to the hypothesis that the federal government used New York City as ground zero for a simulation, military exercise, or staged event were passionate but evasive and did nothing to exclude the possibility.
Let’s review your visceral reactions to my questions about a simulated or staged situation in NYC that may have occurred before your arrival and/or was still occurring when you showed up:
[You repeating my question] “How confident are you that you were not observing a scene that was staged or set-up for you?” You guys! That question tells me to end this interview! I don’t talk with—this is so bizarre. Staged?! Or set up for you? Patients come to me. They’re diaphoretic, sweating, they have x-rays, and they’re hypoxic. How is that staged? I mean, I’ve been taking care of patients my whole career. I was inundated trying to save patients’ lives. Yes, it was all a big stage. What is that question??!?!”
So, you did not answer the question directly or say how confident you were but said you were inundated trying to save patients’ lives, which contradicts what you told me about the number of patients you treated and the patient turnover in New York.
…I cannot even discuss that. It’s so out there. It’s so out there. I have no idea what you’re asking me in [question] number five. It was some sort of simulation? This was a catastrophe. We were–these patients were so sick and dying and filling ICUs. I mean, the first ICU to fill is the main ICU. That’s the one I took over. But there were other ICUs all over the hospitals. They had had to convert a number of wards into ICUs. Um, this was not a simulation.
The ICU you “took over” was full of patients who had been on ventilators for weeks - and all but a few died. If 13 out of 16 patients you encountered upon your arrival died, I agree that is catastrophic, but seeing as you weren’t there when the patients arrived - and you describe patterns and a set-up that fit the possibility of like-ailment precipice patients from within the hospital, care homes, and other places - “simulation” is a fair, if speculative, descriptor.
Because you have a background in medical simulation21 (and medical education and overseeing residents & fellows), I was eager to hear a serious response to that question with a calm and robust explanation of how it could not have possibly been a simulation involving live/almost dead patients but I heard no such thing.
The scenes you described in detail were a blend of what you observed with your own eyes and what you had heard, to the point where someone not reading your words would confuse your experience with the experience other doctors had apparently repeated to you:
“What happened here...is that the initial surge caused so many terrible reports of patients being…” – all of my colleagues, half of ‘em I trained! When I got there, they were exhausted! The stories they were telling me! You guy don’t – ah! I’m getting so tired. I mean, literally we were building, they built out ICUs to take care of all the patients on ventilators. Then they had a floor which we called The Wild West. I’ve never seen that in my career in pulmonary medicine. It was an entire floor-long where everybody was breathless. They were breathing fast, they were on non-invasive ventilators or non-rebreather masks. And they were being monitored with a pulse ox. The pulse oxes were in the hallway so that the nurses and the doctors could see who was dropping and who was dropping severely. It was a bizarre monitored unit, like –and they called it The Wild West there. And so the fact that they had to do that and they had to put really–patients on the precipice of respiratory failure in a regular hospital ward, without ICU monitoring, shows you how stretched the resources were. But maybe that was a simulation exercise. I’m sorry if I’m getting, like, really [indecipherable]. I’m just tired.”
In what ways would a simulation exercise involving live patients be different from what you described? (You didn’t say.) It all sounds incredibly strange to me. You thought so too - and used the word “bizarre”.
Do you remember how Americans were barraged with the language of war - not to mention images, videos, and intended to make us everyone believe New York was under attack? You must, because you agreed with President Trump, Andrew Cuomo, and others when you said, “We are at war with this virus!”
Was it a War Against a Virus — or might it have been a “live” military exercise activated to stage the spread of disease, substantiate a pandemic declaration, deploy the mRNA platform, and hide some things that had been going on/getting worse with mortality among the young and the elderly?
I don’t know for sure and you might not either, but we are both living under elected and appointed federal officials who have told very few (if any) truths about anything regarding the Human Rights Heist of 2020-2022, so let’s not pretend they are incapable of pulling off staged or organized events to cover their sins and accomplish their goals, at our expense.
8. Whatever it was that occurred in New York, you seem either indifferent or averse to the root causes being investigated and the event substantiated.
No bombs were dropped on New York and there is still no hard evidence of any chemical or biological bioweapon being directly released in the subway, hospitals, or anyplace else in the city.
And yet 27,000 New Yorkers are reported to have died — which is very much like the toll of a battle or war, except without names of all the dead, public death records we can examine, pictures or videos suggestive of that number of bodies being handled, or a permanent memorial.
You are not interested in the hospitals being investigated and have moved on. You even said,
“I don’t care or know why New York got hit so hard.”
Well I do (care).
My children’s well-being and my husband’s industry (restaurants) were upended thanks in part to story of New York getting “hit hard” by a spreading deadly pathogen. Millions of American families sustained far worse, as did individuals, communities, and economies around the world. You are one of the few doctors who was speaking “live from New York” in spring 2020 who has become more famous and beloved, thanks in part to good work you’ve done to help patients make better-informed choices about their health. Do you not see that New York City was used to scare the world and justify a coerced & mandated “vaccination”?
Unfortunately, “New York got hit so hard” sounds nothing like a disease and everything like a line from chemical-attack drill script. I have family and acquaintances who have worked in harrowing outbreak and disaster situations involving tragic deaths. They do not speak about their experiences in same the way you speak about what you saw in spring 2020. They are far more burdened and reflect with seriousness and respect and a sense of loss, not heroism or hyperbole.
Because I believe you do care about patients and do care about saving lives, I am left to explain those differences and the many other inconsistencies, discrepancies, and curiosities I describe in this letter as possibly being part of an exercise or situation involving matters deemed integral to national security - one that you are not at liberty to discuss or disclose. I could be wrong.
Thank you again for the time you took to respond to my questions via video.
Regards,
Jessica Hockett
UPDATE: Dr. Kory did not respond to this letter, nor did he acknowledge receipt.
Specific events related to your resignation and departure from UW-Madison are not included because the sequence and circumstances are unclear and involve personnel issues outside the scope of my focus. Your advocacy of Ivermectin, later testimony to the Senate committee, & involvement with the George Floyd case are all noteworthy but largely beyond the timeframe and my interest in the first five months of 2020.
p. 39, The War on Ivermectin
Obtained via freedom of information request from UW-Madison.
You said, “It was the fact that we were treating. It’s because Senator Johnson was really angry that nobody was treating. There was no protocols - that no one was treating. And he came across our organization’s website and he saw that I was the chief of critical care service at the major academic medical center in Wisconsin. So he called me. It wasn’t so much me. It was the fact that we were treating. He wanted to hear more about people treating.”
You said the “three pillars” of MECFS are “fatigue, post-exertion fatigue, and brain fog or cognitive deficits” and that it is “generally associated with mononucleosis” at rates lower than those associated with COVID-19.
One might even speculate that doctors who had been engaged in or were known for such research were enlisted in and elevated during the COVID event on purpose, unbeknownst to them.
As I’m sure you’re aware, ethical breaches in disaster medicine situations in the U.S. have precedent and multiple travel nurses who arrived in New York around the same time you did publicly accused NYC hospital staff of treating patients inhumanely. Mal-treatment is violative of the Hippocratic oath and other professional conduct standards; non-treatment can be as well.
Much like this doctor appears to have done.
Dr. Ioannidis wrote, “The pace of re-opening may differ across locations, depending on their evolving levels of infection, hospital capacity, and population vulnerability structure. While treatment advances and vaccine efforts may be successful eventually, lockdown measures cannot be prolonged until we find treatments and vaccines that save many lives, since such breakthroughs may take a long time (or may even never happen). For example, remdesivir has shown promising results in shortening duration of disease, but no conclusive evidence yet for saving lives.”
I hope we can agree that “huge WhatsApp groups” are subject to all manner of social contagion, groupthink, and competitive one-upsmanship.
You said, "No, the hospital did not allow family members to visit their loved ones. It was all on iPads and we had a team that scheduled meetings, and so, like, every afternoon I was doing video iPad meetings.”
See Figure 14 and Table 1 in “Does New York City Make Any Sense?”
FYI, the Samaritan’s Purse tents in Central Park were underutilized.
Did these people who were “coming in” die?
A later report shows e-cigarette sales continued to rise.
Reports about Seattle’s hospital activity would not have been until late February, at earliest. New York would have been the third week in March or so.
The John Hopkins University dashboard and similar tools attempted to mimic radar.
I asked you about this in January but you chose not to respond, saying, “You know, number five, I’m just tired, I’m not gonna answer it. You guys are sitting in your armchairs looking at data and coming up with theories that I have to try to explain to you why your theories don’t make sense? I can’t do it. I can’t do it. You guys want to keep saying that I have some sort of confirmation bias. It’s just – I can’t do it.”
Overwhelmed by what? You were not overwhelmed with patients in Madison and did not describe to me a high-volume or particularly demanding experience in NYC, despite your emotional and hyperbolic testimony on May 6, 2020. In both locations, you seem to have had more of an oversight role.
From your CV: 2008–2015 Director of Simulation Training–Department of Medicine Beth Israel Medical Center, New York
This is a very well done document, Jessica. You are, respectfully but earnestly, pressing the right questions and supplying all the knowable-at-this-point relevant info to bring to the conversation. I do believe that Dr. Korry is a sincere MD and has suffered a lot professionally for his attempts to treat patients with respiratory distress (in part a problem because they stopped doing so during "Covid", telling patients to go home until they were totally sick so they could get the death protocols in hospitals). This, as I understood you to point out at the end, was a commendable thing he did. He also later came to the realization, which he did not address early on, that the shots were harming a lot of people. Anyone who does that is doing a big service, even if in the end their voices get drowned out by the cartel who run things.
However, I think you are on track with this being a simulation and him, likely unwittingly, being part of it. Sage Hana says this type of thing is "part of the op", calling it "cooling the marks". There is not nearly enough publicly available information to support the claims of a deadly spreading virus - your angle being that this was likely largely fabricated/spillover from previous months, and the fact that we can't have access to public health records that would validate the claims, etc vs. Denis Rancourt (and you say similarly) that the patterns, even if taken at face value, can't be from a virulent, deadly pathogen.
I find your delving into the claims he made vs. his actual experience with Covid patients probing. I had never heard the vaping injury angle before, but it makes sense for the lung damage of young patients conflated as Covid. And, of course, the obvious that there really isn't anything to prove, besides the fraudulent "tests", that this was anything NEW; it could mostly have been flu/pneumonia, and hospicide.
I don't remember the entire exchange with Kory, and didn't watch all of his video response to Jessica et al. But, I'd ask Kory this: why did the New York City area need to fly in people from fairly distant states? Many medical specialists--virology, pulmonary, cardiology, etc.--live between Boston and Richmond.
And, Kory came to Manhattan at a time when stay-at-home orders were in place. Why risk Kory taking the covid virus back to Wisconsin?