
New York City Spring 2020: An Unsubstantiated Mass Casualty Event That Appears Fraudulent & Staged
Narrative of an ongoing investigation

Overview via GoogleNotebookLM AI podcast hosts

In the spring of 2020, New York City reported the biggest non-war mass casualty event in its history: a ~27,000-death increase in eleven weeks.1 Most of the deaths happened in one month’s time, most were blamed on a “novel” coronavirus, and few have been substantiated with basic proof.
A graph of New York deaths shows nothing unusual happening until the federal government declared a national emergency and announced 15 Days to Slow the Spread. Deaths then shot up 740% in 22 days, followed by a sharp drop to normal for the rest of the year.2
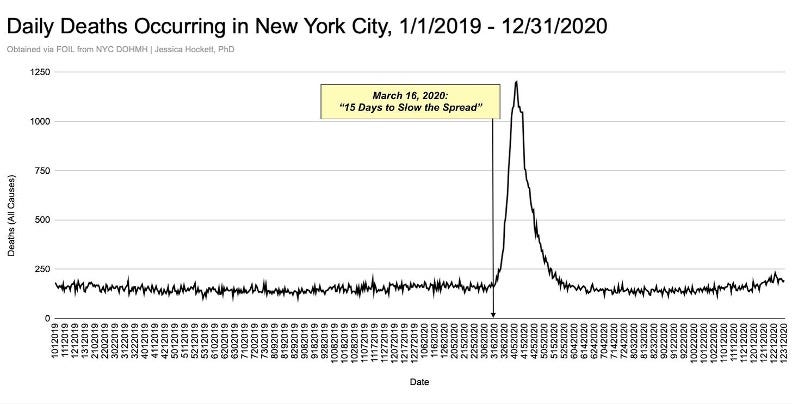
Visually this does not look like a natural event: Eight World Trade Center disaster’s worth of ‘excess death’ in six weeks, with day after day of over 1,000 deaths. Shown this depiction and asked, “What happened here?” no one would say “a disease struck.”3 The dramatic rise and fall is prima facie, intuitively absurd for a contagion. Equally absurd is the idea that the biggest city in America - one of the most iconic and disaster-rehearsed in the world - was somehow “caught off guard” by a cold.
To this day, the official story about what happened in New York in spring 2020 goes something like this:
New York “got hit harder” by a coronavirus.
They didn’t know “how to handle” the virus but learned quickly.
Everyone else learned from New York’s experience. The city “took the hit” first and showed the rest of the world what to do and not do.
The virus “spread” like wildfire in nursing homes because COVID-positive patients were discharged from the hospital into those facilities.
Mistakes were made; things would’ve been worse if there was no “response.”
Thankfully, the government acted “just in time.”4
It’s a story that remains firmly entrenched and largely unchallenged.
Inquiring Mind Wants to Know
I’m not from New York but the death spike has troubled me for a while.

The message we heard from the Chicago area in March 2020 was loud & clear:
New York hospitals are overwhelmed! Don't be New York! Stay home to slow the spread and save lives!
Local and federal authorities pointed to news reports and numbers from America’s biggest city to justify shutting down society and wielding weeks…then months…and then years of harms.
At first I was simply in awe of the sheer speed & number of deaths reported in New York, regardless of what caused the deaths. Later I was surprised that so few people were interested in getting to the bottom of it or going beyond glib explanations that didn’t threaten the government’s pandemic narrative.
After being “permanently suspended” from Twitter for directly quoting The Wall Street Journal, I devoted more time to searching for answers about what could’ve possibly happened. This included trying to find signs of a pathogen or illness in any public time-series data of any kind, such as phone calls to emergency services and deaths by age group, setting, and cause of death.
During suspension, a friend directed me to a Eugyppius article about an insightful analysis from
on the death spikes in the Lombardy region of Italy that preceded the NYC event by a few weeks.5 I’d never heard of Dr. Engler but knew of , the organization which published the analysis, and some of the people associated with it. Engler and an evolutionary biologist used daily death data from provinces in close geographic proximity to show a phenomenon antithetical to what could be expected from a pathogen that spreads from a point-source.The metaphor of an unattended barbecue igniting flames that spread and “build” into a blaze, versus a fireball from the sky suddenly dropping on the forest, captured the illogical proposition I saw in the New York Event but hadn’t been able to articulate. The former scenario, not the latter, is what epidemiologists, disease experts, and the public were led to believe could occur with a pandemic involving something contagious.
Government officials were trained to believe this as well. In a 2005 speech at the National Institutes of Health, U.S. president George W. Bush used the forest fire analogy saying,
"A pandemic is a lot like a forest fire. If caught early, it might be extinguished with limited damage. If allowed to smolder, undetected, it can grow to an inferno that can spread quickly beyond our ability to control it." - George W. Bush
If a ‘pandemic pathogen’ is like a forest fire that starts with a small spark, then why do we see in Lombardy a sudden, very sharp, near-simultaneous rise in deaths in some (but not all) provinces, followed by a staggering drop — as though one or more fireballs struck all at once, spectacularly consumed the forest, and then quickly extinguished?
Why would we ever expect respiratory illness to act like fireballs, asteroids, simultaneous lighting strikes, or similar forces from the natural world - or bombs & so-called ‘bioweapons’ from the artificial world?6
Whether a deadly respiratory disease can "smolder, undetected,” “silently spread,” or transmit between people at all is debatable. But let’s imagine a pathogenic agent were running amok, creating new or added risk of hospitalization or death for some people. Wouldn’t we expect to see gradual, versus sudden, increases in data of various kinds – not something that looks like the Blitz?
Along those lines, I kept searching for “smoke signals” in New York data indicating something unusual was occurring and could, in retrospect, be construed as signs of a new and deadly coronavirus. Without allowing for data manipulation, I saw none.
The idea of a respiratory virus striking a location out of nowhere and killing tens of thousands of people while leaving nearby areas unscathed offends common sense. Why Milan but not Rome?
If latitude/longitude or density matter, how did Berlin and Tokyo and Sydney see no real increase in spring 2020 deaths, while Madrid, London, and Manaus, Brazil saw jumps of 150% or higher?
Modes or speed of travel can’t possibly explain ‘pinpoints’ where the positive tests for the putative pathogen were most prevalent. No epidemiological model accounts for the wildly differential impact in U.S. cities connected by thousands of flights every day. Yet a coronavirus attacking New Orleans while evading Houston and Atlanta and Orlando is precisely what we are supposed to believe happened — and could happen again in the ‘Next Pandemic’.
Iatrogenesis Hypotheses
Upon closer examination of hospital activity and incomplete nursing home death data, I thought it best to approach the “problem” of the New York City event by assuming a novel coronavirus caused no deaths (or no additional deaths), even if that assumption turned out to be wrong.
In 2023, I learned of an early analysis by Denis Rancourt which said a novel spreading virus - novel or otherwise - had not caused first wave deaths spikes but mass homicide by government response:
“I postulate that the ‘COVID peak’ represents an accelerated mass homicide of immune vulnerable individuals, and individuals made more immune-vulnerable, by government and institutional actions, rather than being an epidemiological signature of a novel virus, irrespective of the degree to which the virus is novel from the perspective of viral speciation.” (p. 19)
Of New York, Rancourt said,
“The NYC data makes no epidemiological sense whatsoever. The ‘COVID peak’ here, on its face, cannot be interpreted as a normal viral respiratory disease process in a susceptible population. Local effects, such as importing patients from other jurisdictions or high densities of institutionalized or housed vulnerable people, must be in play, at least.” (p. 16)
Other analysts like Michael Senger and Norman Fenton & Martin Neil used the word iatrogenesis to characterize the cause of many deaths reported in the months following the pandemic declaration.7 Senger’s estimate for death-by-ventilator in New York was too high but he and others like Will Jones of The Daily Sceptic were at least making earnest attempts to discern the number of deaths caused by bad ‘treatments’ versus a novel virus.

I approached it by emphasizing that which can be inferred about how people could and could not have died based on where they died (hospital, care home, personal residence, etc). In this presentation and this comment, I used setting of death to show how iatrogenic measures could have caused or contributed to deaths in New York.

Through further investigation, I realized certain factors I or others had assumed to be culprits or drivers of the death spike were ill-defined, inadequate, unsupported by available data, or fell short of being able to explain or contribute significantly to the toll. This included fear of going to the hospital,8 ventilators, the nursing home policy, remdesivir, and no antibiotics. Darker causes such as high doses of sedatives/paralytics, unilateral DNRs, withdrawing CPR, and high doses of oxygen came into focus - as did signs that the U.S. government (not China) was responsible for allowing, if not purposefully directing, those acts.
I learned that doctors in disaster scenarios are susceptible to making dubious and deadly decisions. It’s hard to deny that 'frontline’ workers in New York and elsewhere crossed the “do no harm” line by following orders, possibly under psychological duress. Hospitals and nursing homes are filled with “damaged ships” that can be sunk at any time, by accident or on purpose. Banning loved ones from healthcare settings increases the risk medical error & preventable death - and reduces the number of witnesses to what’s happening inside.
Given the incredible amount of death in NYC hospitals, the federal government’s failure to order an independent investigation into what happened amounts to depraved indifference.

The Appearance of Fraud
In November 2023, associates and I gave eight reasons we suspected New York data might be false.

Meanwhile, family, friends, and followers constantly asked if I thought the New York curve was ‘true’. Could some of the deaths be purposely faked, or added in error? I wasn’t initially disposed to these possibilities until they became difficult to dismiss. Too many contradictions and conflicts were pointing to a potential distortion of the all-cause death curve.
There is no smoking gun, but I see quite a few bullets that can’t possibly be from the same gun and/or could’ve been placed at scenes before or after the crime. Based on everything I’ve analyzed to date, I believe the curve does not reflect a real-time event - that is, the number of people who are claimed to have died on each day in the places claimed is a misrepresentation in magnitude, timing, or both.
Put simply, I do not see how the New York City death spike can be entirely real and think 2020 daily all-cause curve is manipulated or fraudulent.
Event data are replete with unexpected, disproportionate patterns; incongruences with contemporaneous reports & popular explanations; and discrepancies between the same data from different sources or the same data from the same source. The number & nature of anomalies can’t be ignored.
Some of the more concerning findings which demand immediate explanation from authorities are as follows:
The lack of basic proof (e.g., names, public death records) that ~38,000 people died in two and a half months. City burials9 and records from FEMA on COVID-19 funeral assistance & trucks sent for morgue storage fall short of verifying the total number of casualties.
A staggering increase in deaths among younger, working-age adults (25-54 YO), most of which attributed COVID-19 as underlying cause.
The six-week 250% increase in deaths at Home concurrent to an insufficiently explained out-of-hospital cardiac arrest event.
The cataclysmic number of deaths in hospitals - 22,000 during a period that saw 5,800 in the previous year - amidst a period of decreased hospital activity and patient volume.
Data discrepancies involving the city’s public hospitals and the “epicenter of the epicenter” Elmhurst Hospital.10
No data showing the total number of nursing home/long term care facility residents who died during the timeframe irrespective of place or cause of death – despite multiple investigations and hearings around the Cuomo administration’s so-called “nursing home policy” and attempts to hide the number of nursing home resident COVID deaths.
Disturbing changes and unexpected patterns in ambulance dispatch codes that challenge contemporaneous reports and subsequent studies about what happened with emergency calls and medical services, and why.
The medical examiner’s processing of more than 11,000 deaths in three days at the end of April, with no explanation of why or how that magnitude of processing occurred - and a related records request nearly a year overdue.
Public agency and researcher resistance/refusal to release or provide taxpayer-funded data upon freedom of information or reasonable request.
These and other issues are among those summarized as eleven kinds of serious problems:
I expect to publish a more comprehensive, detailed list of findings drawn from work already released and additional records that raises reasonable doubt as to the veracity of official data & related claims.
New York isn’t the only curve I suspect is manipulated. Based on characteristics of the daily curve, comparisons with New York and Chicago and events like Hurricane Katrina, plus other evidence, I believe Bergamo is fraudulent as well.11
The close match between shape of the New York/Bergamo events and Imperial College projections for the UK and US points to a motive for data engineering: the need for real-life disasters that matched scientists’ predictions. The viruses had to look like bombs going off in a few places in order for people to take directives seriously and obey mandates.
The Appearance of a Staged Event
The New York Event also appears staged.
By ‘staged,’ I mean set-up or presented in the moment or ex post facto to look like something other than what it actually is or was.
A full case for a Staged Event is more difficult and complex to make in a summary for two reasons:
It involves presenting complex qualitative evidence, e.g., news stories, press conferences, obituaries, interviews, pictures, videos, executive orders, documents, timelines, and details about events within the main event, etc.
It’s hard for people to revisit and reinterpret what they saw, heard, and read at the time through an entirely different lens. No one wants to think their government would run a psychological operation against the populace, use healthcare workers to carry out euthanasia protocols, and activate military forces for a mirage — even if it were activated by accident or out of stupidity. The idea is deeply disturbing regardless of which officials or agencies or private parties could have been involved.
Hopefully enough time has passed for people to consider whether watching the ‘reaction’ in New York was any different from watching a Hyper-Reality TV Show: Scenes of people lined up outside a hospital; young doctors insisting they were under siege & feared for their own lives; garbage-bag-wearing nurses; First Responders in gas masks; refrigerator trucks said to be filled with bodies; citizens reporting the incessant sound of sirens; banging posts & pans for ‘frontline’ workers…

…all of it was a perfect fit for the New York backdrop — and critical to the staging of global pandemic triggered by reports of ‘unexplained pneumonia’ in Wuhan, China, and a speedy, incredulous sequence of events.12
Americans were treated to a bi-coastal plot-line, Virus from Afar Coming to Soon to a City Near You, with the Big Apple as the climax. The first COVID “case” in New York City proper was a nurse returning from Iran and came just in time for cautionary tales about the Iranian regime’s failure to take precautions and images of mass burial pits allegedly dug for coronavirus victims.13 Media coverage of death & doom in Iran, northern Italy, and Madrid doubtless primed the city (if not the Western world) for ‘covid’s’ impending arrival.


Scenes “Seen”
Similar to my belief about a fraudulent death curve, I didn’t always see New York as a staged event. The more I revisited words, images, testimonies, and decisions, the harder it became to not see scenes from a theatrical production imitating a chemical warfare attack under the cover of ‘global pandemic’.
It’s no accident New York and federal officials repeatedly invoked the language, analogy, and imagery of war.14 The trucks, the Navy ship, the battle cries for more supplies and help were illogical, overblown responses to the alleged threat posed.15 None of it made sense for a disease outbreak. Aspects of the outsize ‘response’ occurred around the world - like the field hospitals - but New York was presented as America’s Ground Zero and, at minimum, appears to have been used to “practice” military operations and test system capacity for an act of terrorism, foreign invasion or World War III.
The city has a massive emergency management agency, and years of preparedness activities before & since 9/11, yet was immediately presented as caught off guard by a coronavirus and under-resourced (e.g., not enough PPE, tests, ventilators, etc.). On re-examination, posts about supply shortages, being overwhelmed by patient volume/severity, and a “biblical” situation do not look or sound like staff are facing a true crisis.

Nearly every NYC data point hinges around the 15 Days to Slow the Spread announcement - which is reason enough to wonder if it was euphemism that activated a domestic (if not global) drill. Lending credence to the idea a drill was set in motion, not merely a response, Secretary of State Mike Pompeo told the press on March 20th, “We are - we are in a live exercise here.” Exercises are devised around goals and targets. It’s difficult to dismiss as coincidence the New York event increase of ~27,000 deaths being the same as the “minimum scenario” anticipated in a 2008 mass fatality guide for pandemic flu (27,105), and very close to the number Andrew Cuomo yelled at a press conference (26,000).
Voices “in the trenches” also point toward a drill being conducted. It’s easier now than it was at the time to spot themes suggestive of a common script or directed talking points (example 1, example 2). The same is true of various essays and diary-esque articles published in the timeframe (example 1, example 2, example 3). Controlled messaging and messengers are critical to mission execution, public support, and morale. A staged operation mimicking an attack would likewise make sure those speaking to or via mainstream & independent media were singing from the same songbook.

Reports from the “frontline” were intended to demonstrate something very real and very taxing was occurring…but was it?
Should we expect an ER doctor to be doing an interview during the greatest loss of life New York City hospitals have experienced?
Why do National Guardsmen sent to the “epicenter” hospital look more like a softball team than they do a cadre assisting with a calamity? And why did a spokesperson call it a “show” and an “amazing experience”?
How come hospital staff were quickly rewarded with free vacations, giving the impression they may have participated in a simulation without their knowledge or consent?

None of the frontline voices coming from New York challenged the government’s claims about a coronavirus spreading and killing people at home or sending them to the hospital in need of different or repurposed treatments. Some of the most elevated - like Craig Spencer, Colleen Smith, & Cameron Kyle-Siddell - were international crisis and medical simulation specialists. Their elevation in mainstream media was neither organic nor a mistake. Critical care expert Pierre Kory arrived in Manhattan after the death peak and yet was summoned days later to testify about what he was seeing before a U.S. Senate committee. His statements (then and later) sound more like a military maneuver or experiment using real patients than a disease-spread emergency.16
Seemingly genuine firsthand accounts about maltreatment of patients in NYC hospitals from travel nurses surfaced in the later stages of the event. Considering how tightly controlled information was at the time, their stories being permitted on social media - and promoted via videos, books, & appearances - makes little sense and looks like controlled opposition. No formal inquiries of their respective hospitals resulted, which raises questions about the veracity and purpose of their real-time testimonies and subsequent celebrity status.17
Another example of a staged scene evocative of war was Hart Island – the city’s graveyard for unclaimed decedents. Pictures and video footage were used to show America and the world that (like Iran and Italy) New York was overwhelmed with carnage. Data show a six-week increase in burials on the island but comparisons of death records with images in news reports proves most on-camera decedents had not died recently. No other city in the U.S. has a separate, limited-access island for indignant decedent dispositions. The fact a ‘pandemic’ took off in one that does is suspiciously fortuitous.
Scenes Unseen
A staged event is as much about what is NOT seen or heard as much as what is - aka, evidence of absence. Which scenes weren’t observed or aren’t well-documented but should have been? What dogs didn’t bark?
The most compelling ‘unseen scenes’ are images or testimony corroborating the management of 27,000 extra bodies. It would be impossible to hide the task from public view in the age of smartphones. Moving dead weight in a dignified manner calls for incredible manpower. “Who did that work?” asked midwestern farmer Steve Lucie - a simple question the federal government should be able to answer and prove without hesitation. Given the number of hospital inpatient deaths alone, hundreds of doctors, nurses, and other staff should be talking about their experiences and be the subjects of in-depth qualitative study. Where are they? Better yet, where are the researchers who want to hear from them?
We also might expect many New Yorkers being connected to someone who died. Most residents I’ve spoken to do not know anyone who became suddenly ill and needed medical care in those weeks, let alone have a direct acquaintance or relation who perished. With a few exceptions, stories of the dead are more likely to be second or third-hand tales involving a doorman’s mother or cousin’s barber’s grandpa than they are friends or relatives. As far as I can tell, the spectacle was at odds with the vast majority of residents’ ‘lived experiences'.
It’s also at odds with what The New York Times pretended had occurred. Their May 24th ‘Incalculable Loss’ feature was intentionally evocative of a war list and displayed 1,000 (not 100,000) names of dead Americans.18 Only 94 of the names were NYC residents, which is fewer New Yorkers than die on a normal day of any cause.

None of this is to suggest there wasn’t a mass casualty event of significant magnitude, or that iatrogenic measures didn’t kill thousands of people. A “verified” toll derived from FEMA funeral assistance data points to twice the normal number of deaths in eleven weeks. Even if a simulation using existing patients & care home residents activated, some excess could be expected from people who would have died in later weeks or months dying sooner. Who exactly died - and how many - is another matter altogether. Government-dependent populations such as recent immigrants, homeless, mentally-disabled/challenged adults, prisoners, and public housing residents are possibilities, as populations less likely to be ‘missed’ and their deaths easier to double-count or ‘move’ via digital legerdemain.19
“Okay,” some may say, “But if the event was staged and data moved and/or fabricated, there would be whistleblowers. Or you think eight million people are keeping a secret?”
No, not at all.
Authorities created a “closed system event” by rearranging hospitals, redeploying & furloughing staff, bringing in military personnel, banning visitors, and instituting myriad disruptive protocols and policies in healthcare/congregate settings & emergency medical services. This was all done intentionally, in my opinion, and without remorse by those who devised and instituted the measures.
I believe it was democide assisted by full-blown psychological warfare against those charged with saving lives.20

The sudden siloing of systems, agencies, and individuals helped hide what wasn’t happening and ensured that - unlike the World Trade Center disaster - no one person or group of people observed a phenomenon that could have generated the number of deaths purported.
Cases in point: I showed one NYC public hospital doctor the daily all-cause death curve for his facility and asked him if it reflected what he observed. He wasn’t sure. The same was true of an NYPD detective, who told me ambulance data for patients pronounced dead at the scene didn’t match his unit’s experience and would’ve required a staggering amount of overtime work and pay.
In a closed system event, people only know and can speak to what they experienced or did and are not privy to what is happening elsewhere. The most controversial or high-risk aspects of the operation would have been be handled by military and intelligence agencies, so as not to put employees of city-run agencies and hospitals at risk of knowing about or being responsible for too much. While fear, NDAs, bribes/promotions, and other silencing techniques could be in the mix, for me the absence of whistleblowers is better evidence the event didn’t happen as alleged than evidence it did.
If the New York event were a true disaster of the magnitude purported, five years later, we might also expect things like
a permanent memorial commemorating the event or the decedents,
documentaries featuring the harrowing testimonies & recollections of doctors, nurses, first responders, and medical examiner’s staff.
a federal commission or inquiry focused on what happened in those eleven weeks, and
class-action lawsuits against hospitals and other city services.
We would not expect dynamic silence.
The simplest explanation for the silence is that the depictions in spreadsheets & on screens are intentional distortions of on-the-ground realities.
Why Does the New York Event Matter?
Many outrageous and idiotic things happen in New York City all the time - things that happen no place else in the country or world and should have no bearing on how anyone except New Yorkers live their lives. Unfortunately, being the nation’s media capital & financial center, the rest of us are often “forced” to pay attention to a good number of these occurrences as urgent matters BECAUSE they are in New York.
In spring 2020, not only the United States but much of the world paid the price of staged panic and a staged ‘outbreak’ in the city that doesn’t sleep. It is very hard to imagine Americans, at least, believing the globe was beset with a dangerous viral threat without it seeming to ‘attack’ New York — just like in the movies.

Beacuse if a spreading virus doesn’t spread-to-kill in one of the globe’s densest cities, what kind of a spreading virus is it? Not one worth a front-page headline, let alone a complete upending of society and widespread shutdowns.
Whether real, imagined, or some combination thereof, the New York City death spike undoubtedly helped to
verify the existence of a new cause of death wrought by a new pathogenic agent,
substantiate a pandemic declaration,
close schools, churches/places of worship, restaurants/gathering places, & businesses,
halt weddings, funerals, baptisms, bar mitzvahs, quinceañeras, and other rituals that mark the beginning, sustaining, and ending of life,
legitimize a national emergency decree & unprecedented activation of the Stafford Act in all 50 states,
cast the specter of a coronavirus suddenly spreading and adding risk of severe illness and death to certain groups of people,
sell the world on the need for repurposed and unique treatments,
scare/compel/coerce the populace into getting a dedicated “vaccine,”
justify decades of pandemic/bioterrorism preparedness,
rationalize funding/resources toward preparing for “the next pandemic,” and
reify "dangerous" gain-of-function research & viral agents allegedly resulting therefrom.
Making ‘the pandemic’ there was making ‘the pandemic’ everywhere.
A Mass Illusion Event in the Digital Age wouldn’t require tens of thousands of people actually-dying on the days claimed. Only some would need to—with the world needing to believe the rest had.

Post subject to updates, revisions, and fixes. Substantive changes and significant errors will be noted.
Compared to the same weeks in 2019 (Source: CDC WONDER)
Increase is baseline to peak.
For a sense of what people say when given the one-month number, see this February 2023 tweet.
From What Happened in New York City in Spring 2020? IPAK Science Director’s Webinar
My comments at the time were not NYC-specific and show I was thinking of SARS-CoV-2 and the possibilities of a U.S. lab leak differently than I do now. My current views on ‘origins’ can be found on this page.
Todd Kenyon put it well when he showed a similar pattern in place of death data for the UK, “There is no path of [natural] spread. It’s everywhere all at once.”
Other people had used iatrogenic on Twitter but Senger is the first I remember using it in an article related to my interests.
Contradicted by 911 call and ambulance dispatch data — and challenged by redirection of calls to telemedicine and (in some cases) temporary reclassification of visits to the ED as visits to outpatient stations.
City burials means unclaimed decedents who were buried on Hart Island.
The Greater NYC/Tri-State area, London, Madrid, Barcelona, other provinces in Lombardy, are also suspiciously high and a focus of mass propaganda & militarized operations.
Explained well by Nick Hudson and shown in a timeline from @theotherphilipp.
The war metaphor was early and global - not confined to the U.S., but New York was (arguably) the site of the most prolifically-documented “battle” in a single location.
The number of ventilators Mayor DeBlasio said New York City needed (15,000) was equivalent to 75% of all hospital beds — an illogical projection disproportional to any demonstrated need.
Nicole Sirotek was at Lincoln Medical Center and Nurse Erin at Elmhurst.
Normal was 50K-60K Americans each week.
My attempts to obtain ambulance records related to this possibly have been unsuccessful. See FDNY Suddenly Closes My FOIL Request for Ambulance Transfer Data
The basic mechanics of executing Democide under the guise of a pandemic/epidemic are outlined in this thread.
I recall screaming incoming and easily avoidable iatrogenic democide or just iatrocide at the top of my lungs throughout 2020/21 and many of the fake-awake Sophists that went on to "lead" the "resistance" claiming to not know what those words meant.
Facebook banned me for over a year for simply posting those two former words with their dictionary definition in late March 2020, along with a few piano chords of Star Wars and the reminder that we're all that's left of the rebels now and that stormtroopers can't shoot for shit.
I probably would have added a fist bump emoji.
Most of these people we've both intersected with are not playing straight or they're absolute incentivized morons that are being artificially promoted imho.
None of what has transpired was a complex problem to decipher, albeit there remains a complex problem to be tackled which few are fit to fight, you're one of them imho (fist bump emoji/Chewie affirmative grunt)
"the dogs that didn't bark"
OMG. yes. ESPECIALLY the documentaries!! Hell we got NEW documentaries on JonBenet Ramsey and Menendez brothers but NOTHING on New york "heroes"?
I'm very suspicious of MO NH "covid cases" let alone deaths having seen first hand how tests were done regardless of symptoms (still want to know just what the hell "asymptomatic covid" is!). No one is investigating the FRAUD hospitals did on applying covid tests to every patient...and how many were 'positive' without symptoms
Wonder if there is any way to to try to find travel nurses who worked in NYC at the time. I know a few travel RN's and I'll be asking if they know any NYC nurses during that time. Time to play "6 degrees of Kevin Bacon"